Rural Department of Community Health, La Trobe Rural Health School, La Trobe University, Bendigo, Victoria, Australia.
Department of Rural Health, Faculty of Medicine, Dentistry and Health Sciences, University of Melbourne, Shepparton, Australia.
PLoS One. 2022 Mar 17;17(3):e0265559. doi: 10.1371/journal.pone.0265559. eCollection 2022.
It is unclear which Early Warning System (EWS) score best predicts in-hospital deterioration of patients when applied in the Emergency Department (ED) or prehospital setting.
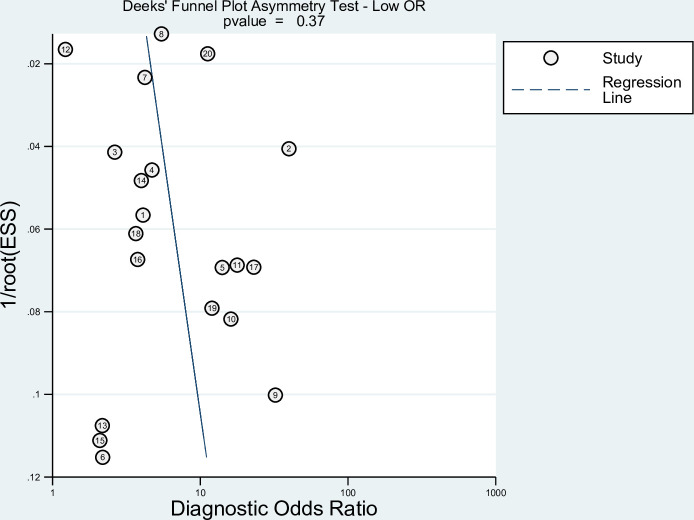
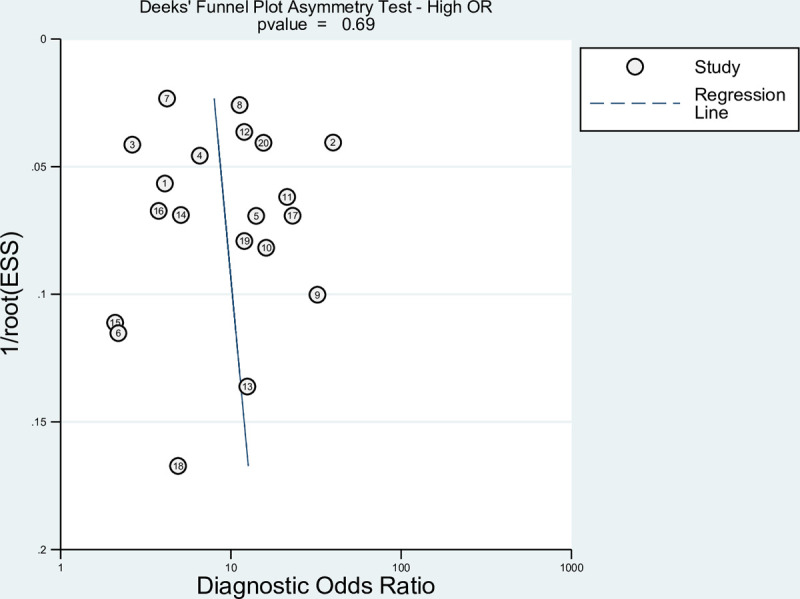
This systematic review (SR) and meta-analysis assessed the predictive abilities of five commonly used EWS scores (National Early Warning Score (NEWS) and its updated version NEWS2, Modified Early Warning Score (MEWS), Rapid Acute Physiological Score (RAPS), and Cardiac Arrest Risk Triage (CART)). Outcomes of interest included admission to intensive care unit (ICU), and 3-to-30-day mortality following hospital admission. Using DerSimonian and Laird random-effects models, pooled estimates were calculated according to the EWS score cut-off points, outcomes, and study setting. Risk of bias was evaluated using the Newcastle-Ottawa scale. Meta-regressions investigated between-study heterogeneity. Funnel plots tested for publication bias. The SR is registered in PROSPERO (CRD42020191254).
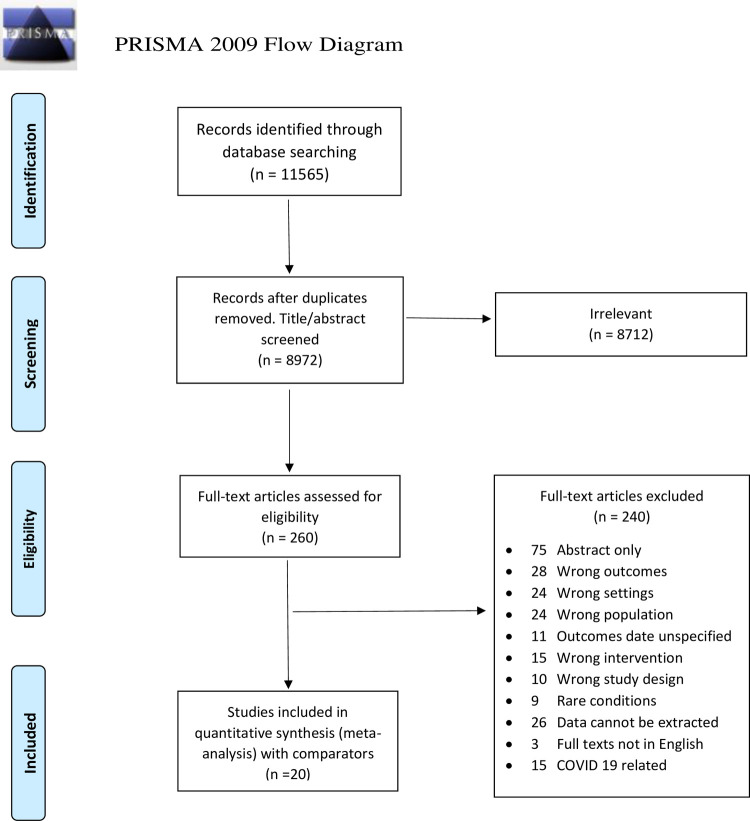
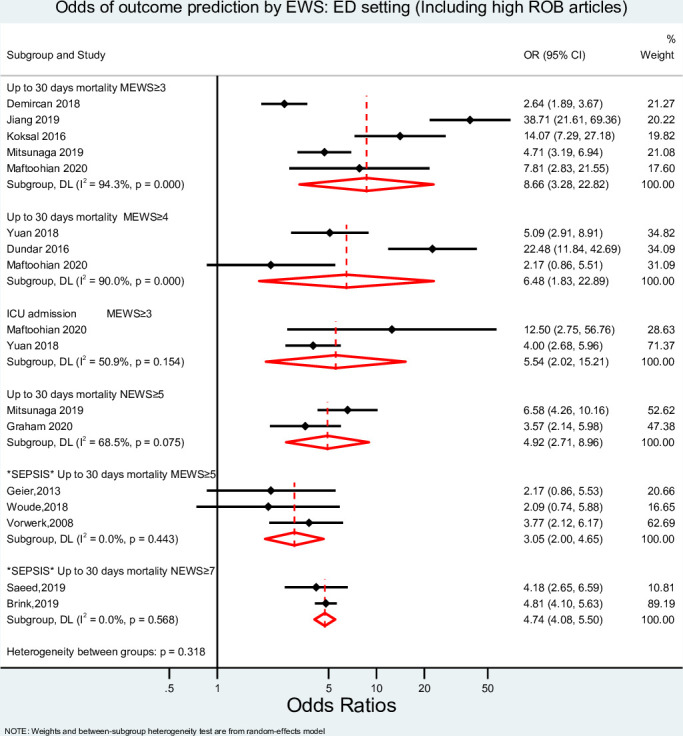
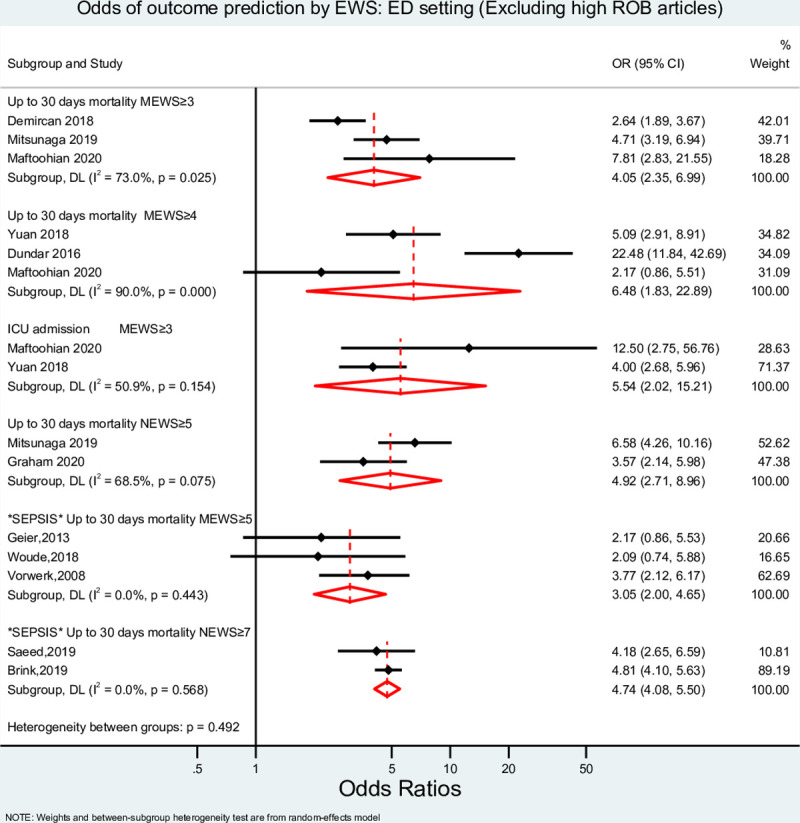
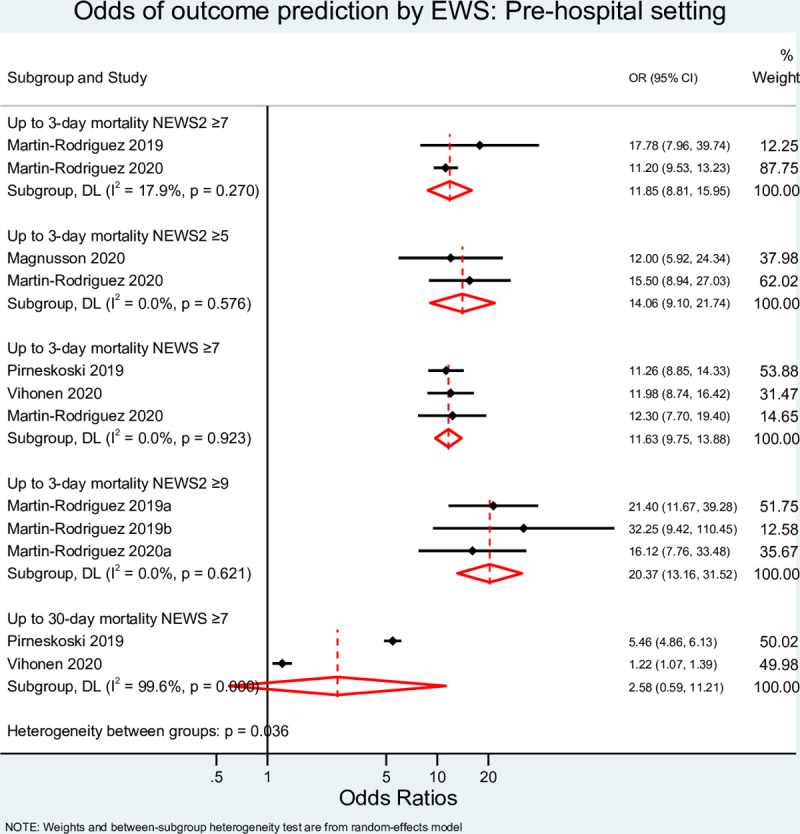
Overall, 11,565 articles were identified, of which 20 were included. In the ED setting, MEWS, and NEWS at cut-off points of 3, 4, or 6 had similar pooled diagnostic odds ratios (DOR) to predict 30-day mortality, ranging from 4.05 (95% Confidence Interval (CI) 2.35-6.99) to 6.48 (95% CI 1.83-22.89), p = 0.757. MEWS at a cut-off point ≥3 had a similar DOR when predicting ICU admission (5.54 (95% CI 2.02-15.21)). MEWS ≥5 and NEWS ≥7 had DORs of 3.05 (95% CI 2.00-4.65) and 4.74 (95% CI 4.08-5.50), respectively, when predicting 30-day mortality in patients presenting with sepsis in the ED. In the prehospital setting, the EWS scores significantly predicted 3-day mortality but failed to predict 30-day mortality.
EWS scores' predictability of clinical deterioration is improved when the score is applied to patients treated in the hospital setting. However, the high thresholds used and the failure of the scores to predict 30-day mortality make them less suited for use in the prehospital setting.
目前尚不清楚哪种早期预警系统(EWS)在急诊科(ED)或院前环境中应用时,能最好地预测患者的院内恶化。
本系统评价(SR)和荟萃分析评估了五种常用 EWS 评分(国家早期预警评分(NEWS)及其更新版本 NEWS2、改良早期预警评分(MEWS)、快速急性生理学评分(RAPS)和心脏骤停风险分诊(CART))的预测能力。感兴趣的结局包括入住重症监护病房(ICU)和住院后 3 至 30 天的死亡率。使用 DerSimonian 和 Laird 随机效应模型,根据 EWS 评分切点、结局和研究环境计算汇总估计值。使用纽卡斯尔-渥太华量表评估偏倚风险。元回归分析了研究间异质性。漏斗图检验发表偏倚。SR 在 PROSPERO(CRD42020191254)中注册。
总共确定了 11565 篇文章,其中 20 篇被纳入。在 ED 环境中,MEWS 和 NEWS 在 3、4 或 6 分的切点具有相似的预测 30 天死亡率的汇总诊断比值比(DOR),范围从 4.05(95%置信区间(CI)2.35-6.99)到 6.48(95% CI 1.83-22.89),p = 0.757。MEWS 在切点≥3 时预测 ICU 入住的 DOR 相似(5.54(95% CI 2.02-15.21))。MEWS≥5 和 NEWS≥7 预测 ED 中脓毒症患者 30 天死亡率的 DOR 分别为 3.05(95% CI 2.00-4.65)和 4.74(95% CI 4.08-5.50)。在院前环境中,EWS 评分显著预测 3 天死亡率,但未能预测 30 天死亡率。
当将评分应用于在医院环境中治疗的患者时,EWS 评分对临床恶化的预测能力得到提高。然而,由于评分使用的高阈值以及评分未能预测 30 天死亡率,使得它们不太适合在院前环境中使用。