Department of Family Medicine, McGill University, Montreal, Quebec, Canada.
Lady Davis Institute for Medical Research, Jewish General Hospital, Quebec, Montreal, Canada.
BMC Health Serv Res. 2022 Mar 17;22(1):353. doi: 10.1186/s12913-022-07672-5.
Many primary care sites have implemented models to improve detection, diagnosis, and management of dementia, as per Canadian guidelines. The aim of this study is to describe the responses of clinicians, managers, and staff of sites that have implemented these models when presented with audit results, their insights on the factors that explain their results, their proposed solutions for improvement and how these align to one another.
One audit and feedback cycle was carried out in eight purposefully sampled sites in Ontario, Canada, that had previously implemented dementia care models. Audit consisted of a) chart review to assess quality of dementia care indicators, b) questionnaire to assess the physicians' knowledge, attitudes and practice toward dementia care, and c) semi-structured interviews to understand barriers and facilitators to implementing these models. Feedback was given to clinicians, managers, and staff in the form of graphic and oral presentations, followed by eight focus groups (one per site). Discussions revolved around: what audit results elicited more discussion from the participants, 2) their insights on the factors that explain their audit results, and 3) solutions they propose to improve dementia care. Deductive content and inductive thematic analyses, grounded in causal pathways models' theory was performed.
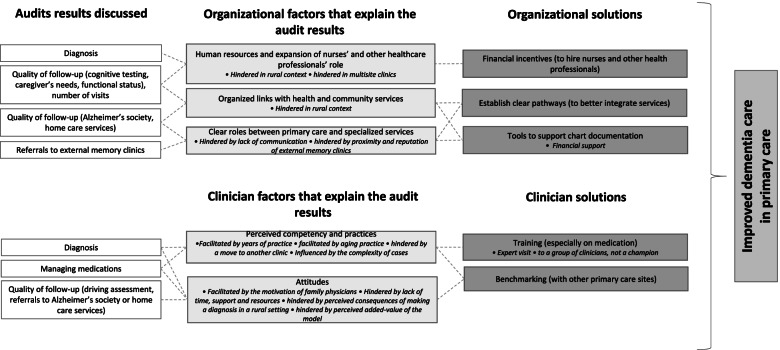
The audit and feedback process allowed the 63 participants to discuss many audit results and share their insights on a) organizational factors (lack of human resources, the importance of organized links with community services, clear roles and support from external memory clinics) and b) clinician factors (perceived competency practice and attitudes on dementia care), that could explain their audit results. Participants also provided solutions to improve dementia care in primary care (financial incentives, having clear pathways, adding tools to improve chart documentation, establish training on dementia care, and the possibility of benchmarking with other institutions). Proposed solutions were well aligned with their insights and further nuanced according to contextual details.
This study provides valuable information on solutions proposed by primary care clinicians, managers, and staff to improve dementia care in primary care. The solutions are grounded in clinical experience and will inform ongoing and future dementia strategies.
许多初级保健场所已经按照加拿大指南实施了模型,以提高痴呆症的检测、诊断和管理水平。本研究的目的是描述实施这些模型的场所的临床医生、管理人员和工作人员在收到审计结果时的反应,他们对解释结果的因素的看法,他们提出的改进方案,以及这些方案之间的一致性。
在加拿大安大略省的 8 个有针对性地选取的、之前实施过痴呆症护理模式的场所进行了一个审计和反馈循环。审计包括:a)评估痴呆症护理指标质量的病历审查,b)评估医生对痴呆症护理的知识、态度和实践的问卷,c)了解实施这些模式的障碍和促进因素的半结构化访谈。以图形和口头陈述的形式向临床医生、管理人员和工作人员提供反馈,然后进行 8 个焦点小组(每个地点 1 个)讨论。讨论围绕以下内容展开:a)审计结果引发参与者更多讨论的内容,b)他们对解释审计结果的因素的看法,以及 c)他们提出的改善痴呆症护理的方案。采用基于因果路径模型理论的演绎内容分析和归纳主题分析。
审计和反馈过程使 63 名参与者能够讨论许多审计结果,并分享他们对以下因素的看法:a)组织因素(人力资源不足,与社区服务建立有组织联系的重要性,明确的角色和外部记忆诊所的支持)和 b)临床医生因素(对痴呆症护理的感知能力实践和态度),这些因素可以解释他们的审计结果。参与者还提出了改善初级保健中痴呆症护理的方案(经济激励措施、建立明确的途径、添加工具以改善图表记录、开展痴呆症护理培训,以及与其他机构进行基准测试的可能性)。提出的解决方案与他们的见解很好地一致,并根据具体情况进一步细化。
本研究提供了有关初级保健临床医生、管理人员和工作人员为改善初级保健中的痴呆症护理而提出的解决方案的宝贵信息。这些解决方案基于临床经验,将为正在进行和未来的痴呆症策略提供信息。