Department of Gastroenterology and Hepatology, Musashino Red Cross Hospital, Musashino-shi, Japan.
Department of Gastroenterology and Hepatology, Tokyo Medical Dental University, Bunkyo-Ku, Japan.
Cancer Rep (Hoboken). 2022 Nov;5(11):e1613. doi: 10.1002/cnr2.1613. Epub 2022 Mar 18.
Therapeutic strategies for unresectable hepatocellular carcinoma (u-HCC) in geriatric patients are important for real-world practice. However, there remain no established biomarkers or therapeutic strategies regarding the best second-line agent after atezolizumab plus bevacizumab therapy.
In this study, we investigated the usefulness of modified Geriatric 8 (mG8) score in examining elderly patients (≥75 years old) with unresectable hepatocellular carcinoma (u-HCC) using sorafenib or lenvatinib as first-line therapy.
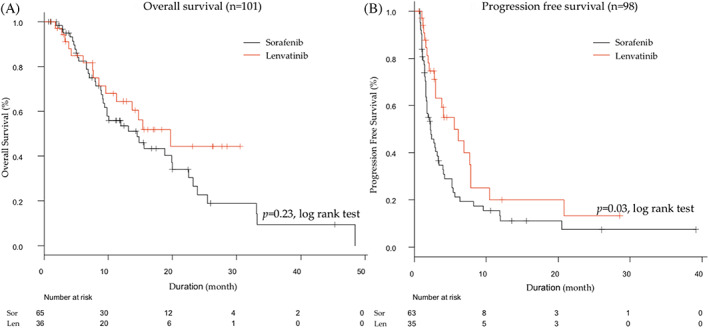
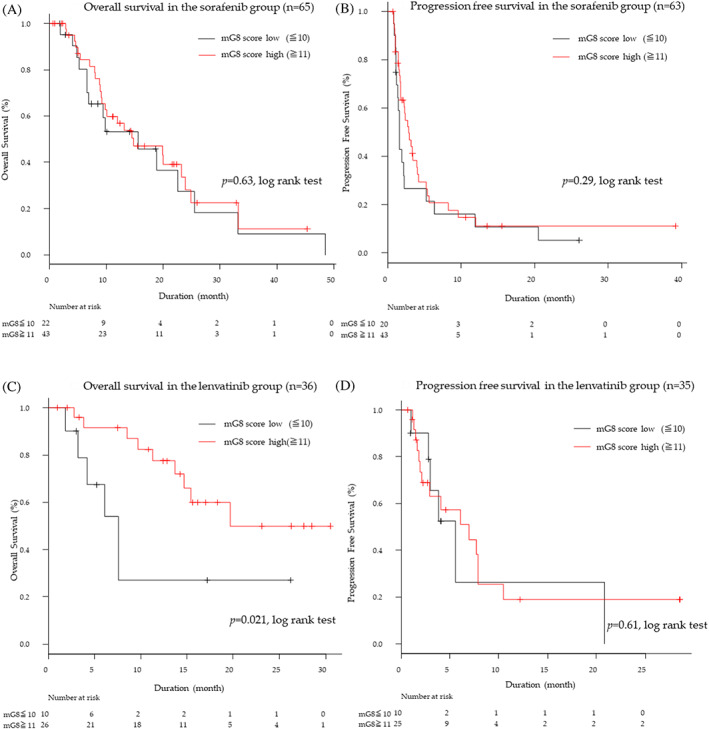
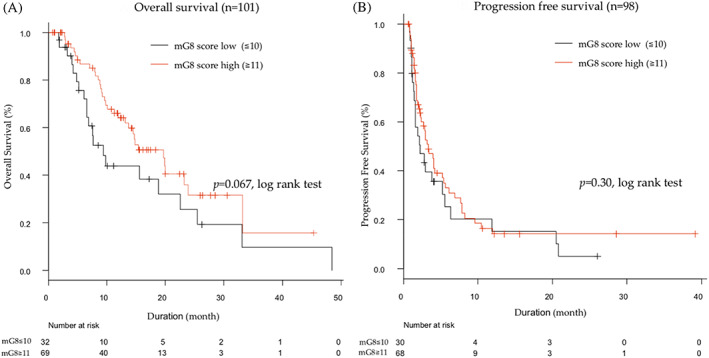
This study assessed 101 elderly patients with u-HCC for their mG8 score (excluding elements of age from 8 items) and classified them into 2 groups according to their mG8 score: ≥11 as the high-score group and ≤ 10 as the low-score group. Among those taking sorafenib, no significant differences were noted in overall survival (OS) and progression free survival (PFS) between low and high mG8 score groups. Only modified albumin-bilirubin (ALBI) grade (2b/3 vs. 1/2a: HR 0.34; 95% CI, 0.17-0.69; p = .0029) was significantly associated with OS. Among those taking lenvatinib, patients with a high mG8 score (n = 26) had longer survival than those with a low mG8 score (n = 10) (20.0 months vs. 7.7 months: HR 0.31, 95% CI 0.11-0.89; p = .029). Intrahepatic tumor volume (<50% vs. ≥50%: HR 16.7; 95% CI, 1.71-163; p = .016) and α-fetoprotein (AFP) (<400 vs. ≥400: HR 3.38; 95% CI 0.84-19.7; p = .031) remained significant factors independently associated with OS.
The mG8 score may contribute to making a decision when considering either sorafenib or lenvatinib as a treatment option for u-HCC in elderly patients.
对于老年不可切除肝细胞癌(u-HCC)患者,治疗策略对于实际情况非常重要。然而,在阿替利珠单抗联合贝伐珠单抗治疗后,哪种二线药物是最佳选择,目前仍没有明确的生物标志物或治疗策略。
本研究旨在探讨改良老年 8 项评分(mG8)在评估接受索拉非尼或仑伐替尼作为一线治疗的不可切除肝细胞癌(u-HCC)老年(≥75 岁)患者中的作用。
本研究对 101 例 u-HCC 老年患者的 mG8 评分(不包括 8 项中与年龄相关的项目)进行评估,并根据 mG8 评分将其分为两组:mG8 评分≥11 为高分组,mG8 评分≤10 为低分组。在接受索拉非尼治疗的患者中,低分组和高分组的总生存期(OS)和无进展生存期(PFS)无显著差异。仅改良白蛋白-胆红素(ALBI)分级(2b/3 级与 1/2a 级:HR 0.34;95%CI,0.17-0.69;p=0.0029)与 OS 显著相关。在接受仑伐替尼治疗的患者中,mG8 评分较高的患者(n=26)的生存时间长于 mG8 评分较低的患者(n=10)(20.0 个月比 7.7 个月:HR 0.31,95%CI 0.11-0.89;p=0.029)。肝内肿瘤体积(<50%比≥50%:HR 16.7;95%CI,1.71-163;p=0.016)和甲胎蛋白(AFP)(<400ng/ml 比≥400ng/ml:HR 3.38;95%CI,0.84-19.7;p=0.031)仍是 OS 的独立显著相关因素。
mG8 评分可能有助于在考虑为老年 u-HCC 患者选择索拉非尼或仑伐替尼治疗时做出决策。