Orthopaedic Research Lab, Radboud Institute for Health Sciences, Radboud University Medical Center, Nijmegen, The Netherlands.
Department of Radiotherapy, Radboud Institute for Health Sciences, Radboud University Medical Center, Nijmegen, The Netherlands.
PLoS One. 2022 Mar 18;17(3):e0265524. doi: 10.1371/journal.pone.0265524. eCollection 2022.
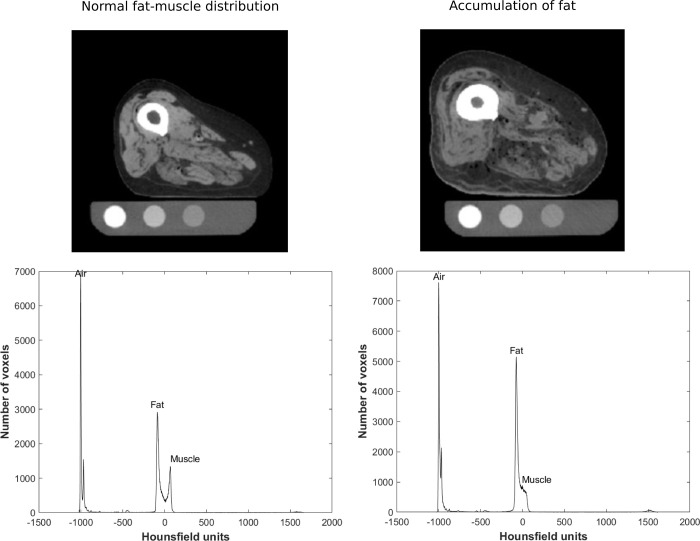
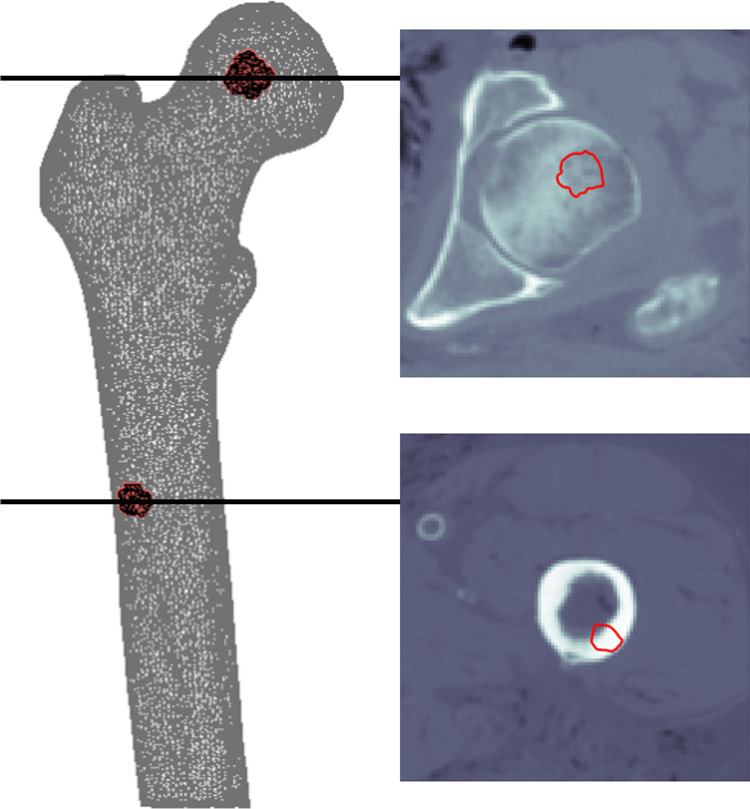
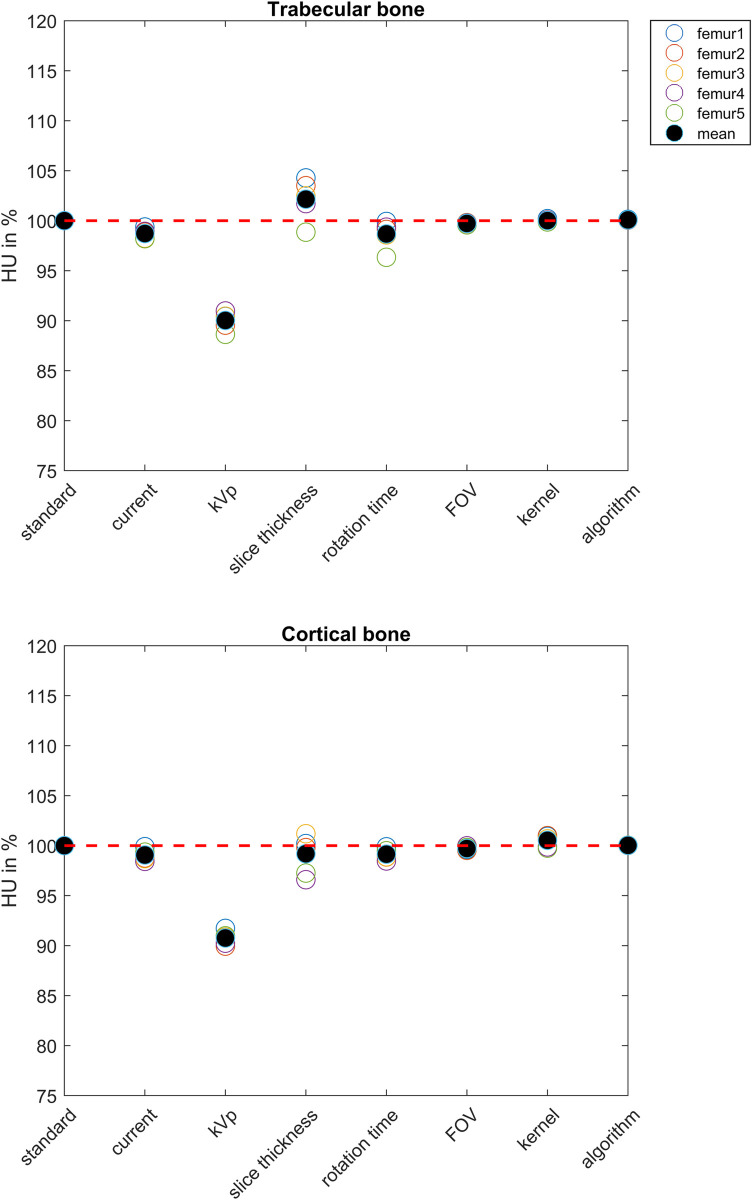
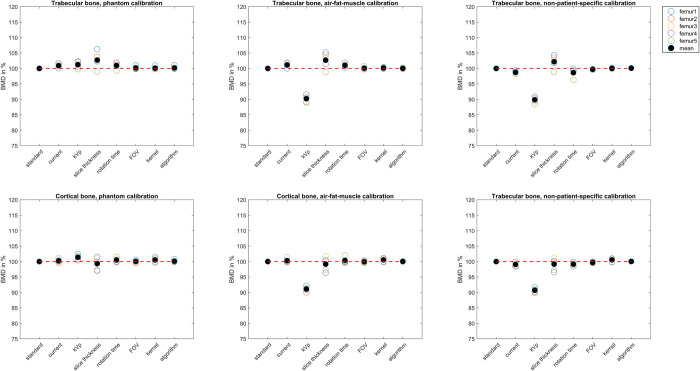
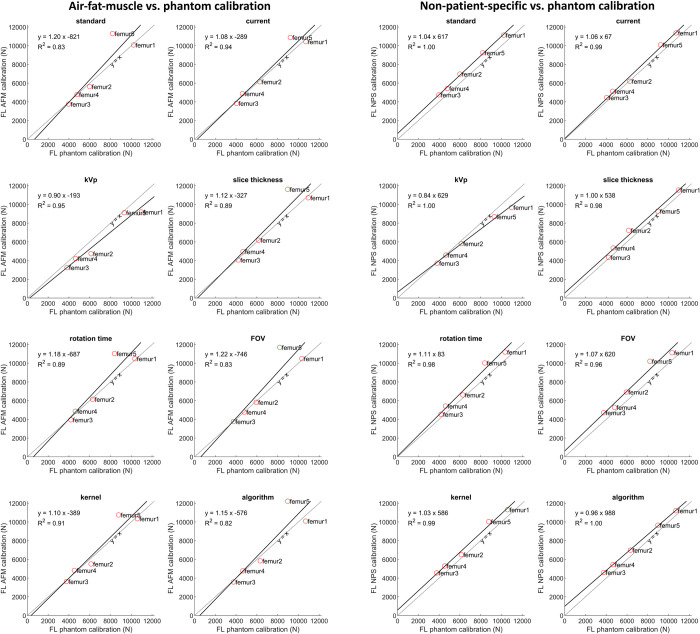
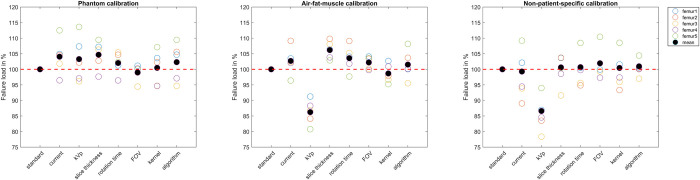
Recently, it was shown that fracture risk assessment in patients with femoral bone metastases using Finite Element (FE) modeling can be performed using a calibration phantom or air-fat-muscle calibration and that non-patient-specific calibration was less favorable. The purpose of this study was to investigate if phantomless calibration can be used instead of phantom calibration when different CT protocols are used. Differences in effect of CT protocols on Hounsfield units (HU), calculated bone mineral density (BMD) and FE failure loads between phantom and two methods of phantomless calibrations were studied. Five human cadaver lower limbs were scanned atop a calibration phantom according to a standard scanning protocol and seven additional commonly deviating protocols including current, peak kilovoltage (kVp), slice thickness, rotation time, field of view, reconstruction kernel, and reconstruction algorithm. The HUs of the scans were calibrated to BMD (in mg/cm3) using the calibration phantom as well as using air-fat-muscle and non-patient-specific calibration, resulting in three models for each scan. FE models were created, and failure loads were calculated by simulating an axial load on the femur. HU, calculated BMD and failure load of all protocols were compared between the three calibration methods. The different protocols showed little variation in HU, BMD and failure load. However, compared to phantom calibration, changing the kVp resulted in a relatively large decrease of approximately 10% in mean HU and BMD of the trabecular and cortical region of interest (ROI), resulting in a 13.8% and 13.4% lower failure load when air-fat-muscle and non-patient-specific calibrations were used, respectively. In conclusion, while we observed significant correlations between air-fat-muscle calibration and phantom calibration as well as between non-patient-specific calibration and phantom calibration, our sample size was too small to prove that either of these calibration approaches was superior. Further studies are necessary to test whether air-fat-muscle or non-patient-specific calibration could replace phantom calibration in case of different scanning protocols.
最近的研究表明,使用有限元(FE)模型对股骨转移瘤患者进行骨折风险评估,可以使用校准体模或空气-脂肪-肌肉校准进行,而非患者特异性校准效果较差。本研究旨在探讨在使用不同 CT 协议时,是否可以使用无校准体模替代校准体模进行校准。研究了不同 CT 协议对校准体模和两种无校准体模校准方法的 Hounsfield 单位(HU)、计算骨密度(BMD)和 FE 失效负载的影响。将 5 个人体下肢标本放置在校准体模上,根据标准扫描协议进行扫描,并额外扫描了 7 种常用的偏离协议,包括当前、峰值千伏(kVp)、切片厚度、旋转时间、视野、重建核和重建算法。使用校准体模以及空气-脂肪-肌肉和非患者特异性校准对扫描的 HU 值进行了校准,从而为每个扫描生成了三个模型。通过模拟股骨的轴向载荷创建了 FE 模型,并计算了失效负载。比较了三种校准方法在所有协议下的 HU 值、计算的 BMD 和失效负载。不同的协议在 HU 值、BMD 和失效负载方面显示出很小的差异。然而,与校准体模相比,改变 kVp 会导致感兴趣区(ROI)的小梁和皮质区的平均 HU 值和 BMD 分别降低约 10%,使用空气-脂肪-肌肉和非患者特异性校准时,失效负载分别降低 13.8%和 13.4%。结论是,虽然我们观察到空气-脂肪-肌肉校准与校准体模校准以及非患者特异性校准与校准体模校准之间存在显著相关性,但我们的样本量太小,无法证明这两种校准方法中的任何一种都更优。需要进一步的研究来测试在不同扫描协议的情况下,空气-脂肪-肌肉或非患者特异性校准是否可以替代校准体模。