Lei Wei-Te, Chang Ling-Sai, Zeng Bing-Yan, Tu Yu-Kang, Uehara Ritei, Matsuoka Yutaka J, Su Kuan-Pin, Lee Pi-Chang, Cavalcante Joao L, Stubbs Brendon, Lin Pao-Yen, Wu Yi-Cheng, Hsu Chih-Wei, Chen Tien-Yu, Chen Yen-Wen, Yeh Pin-Yang, Sun Cheuk-Kwan, Tseng Ping-Tao, Kao Yu-Hsuan
Section of Immunology, Rheumatology, and Allergy Department of Pediatrics, Hsinchu Mackay Memorial Hospital, Hsinchu, Taiwan; Graduate Institute of Clinical Medical Sciences, College of Medicine, Chang Gung University, Taoyuan, Taiwan.
Department of Pediatrics, Kaohsiung Chang Gung Memorial Hospital, Chang Gung University College of Medicine, Kaohsiung, Taiwan.
EBioMedicine. 2022 Apr;78:103946. doi: 10.1016/j.ebiom.2022.103946. Epub 2022 Mar 17.
Although the current consensus recommends a standard treatment of high-dose intravenous immunoglobulin with high-dose aspirin to manage Kawasaki disease (KD), the use of different adjunctive therapies remains controversial. The aim of the current network meta-analysis (NMA) was to compare the efficacy and tolerability of different existing interventions for the initial and refractory stages of KD.
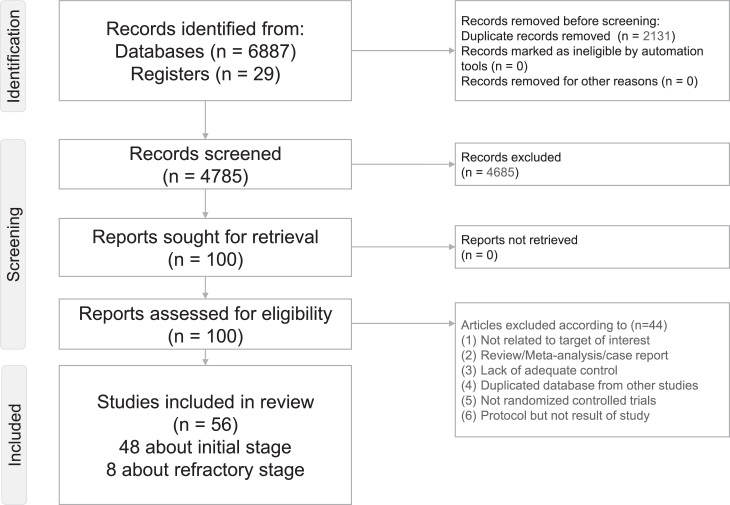
An NMA of randomised controlled trials (RCTs) was conducted using the frequentist model applied after electronic searches in PubMed, Embase, ScienceDirect, ProQuest, ClinicalTrials.gov, ClinicalKey, Cochrane CENTRAL, and Web of Science. The main outcomes were reduced fever duration/diminished severity of fever subsided. The initial stage of KD was defined as the first stage to treat patients with KD; the refractory stage of KD represents KD patients who failed to respond to standard KD treatment. The cut-off points for intravenous immunoglobulin (IVIG) were low (100-400 mg), medium (1 g), and high (at least 2 g).
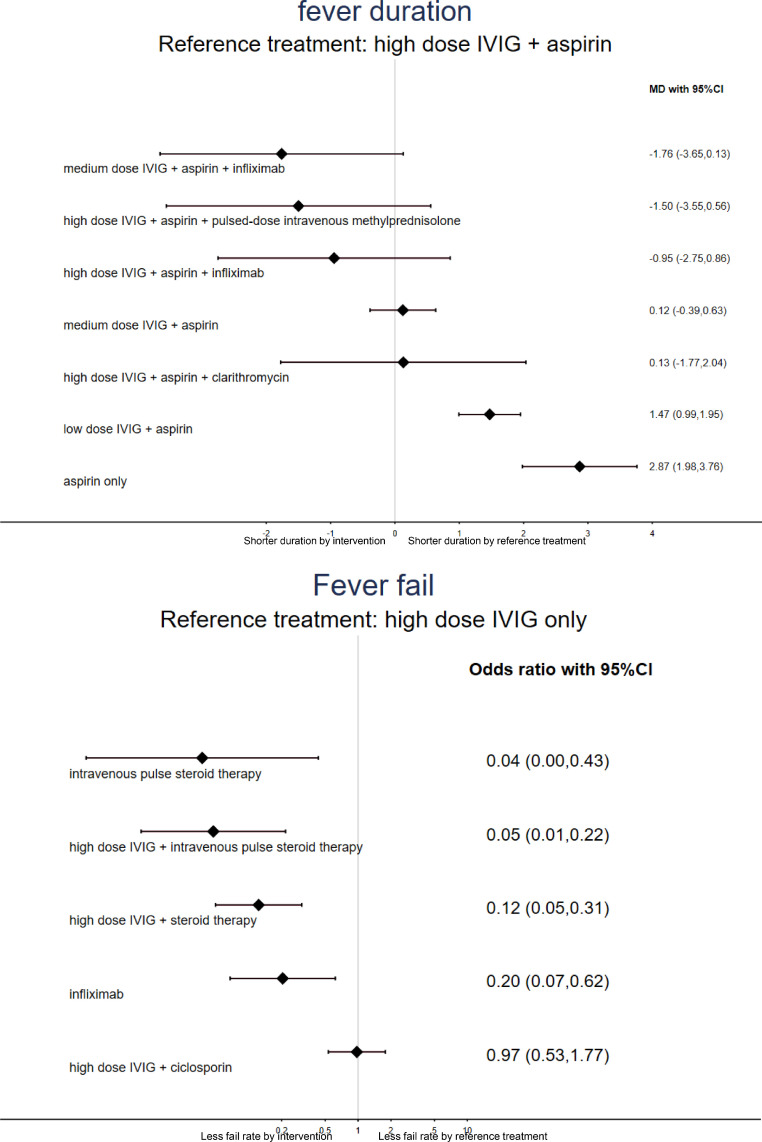
A total of fifty-six RCTs with 6486 participants were included. NMA demonstrated that the medium-dosage IVIG + aspirin + infliximab [mean difference=-1.76 days (95% confidence intervals (95% CIs): -3.65 to 0.13 days) compared to high-dosage IVIG + aspirin] exhibited the shortest fever duration; likewise, the medium-dosage IVIG + aspirin + infliximab [odds ratio (OR)=0.50, 95% CIs: 0.18-1.37 compared to high-dosage IVIG + aspirin] exhibited the smallest incidence of coronary artery lesion (CAL) in the initial-stage KD. In the refractory-stage KD, the high-dosage IVIG + pulse steroid therapy (OR=0.04, 95% CIs: 0.00-0.43 compared to the high-dosage IVIG only) had the best rate of decline of fever; likewise, the high-dosage IVIG + ciclosporin [OR=0.05 (95% CIs: 0.00-1.21) compared to the high-dosage IVIG only] exhibited the smallest incidence of CAL. Infliximab significantly improved resolution compared to the high-dosage IVIG only group (OR=0.20, 95%CIs: 0.07-0.62) in refractory-stage KD.
The NMA demonstrated that the combination therapy with the standard therapy of IVIG and aspirin might have an additional effect on shortening the duration of fever and lowering the CAL incidence rate in patients with acute KD. Moreover, the combination therapy with high-dose IVIG and pulse steroid therapy or cyclosporine therapy might have an additional effect on improving the rate of decline of fever and lowering the incidence rate of CAL in children with refractory KD. Because some of the findings of this NMA should be considered hypothesis-generating rather than confirmatory, further evidence from de novo randomised trials is needed to support our results.
None.
尽管目前的共识推荐采用大剂量静脉注射免疫球蛋白联合大剂量阿司匹林的标准疗法来治疗川崎病(KD),但不同辅助疗法的使用仍存在争议。本网络荟萃分析(NMA)的目的是比较KD初始阶段和难治阶段不同现有干预措施的疗效和耐受性。
采用频率学派模型对随机对照试验(RCT)进行NMA,在PubMed、Embase、ScienceDirect、ProQuest、ClinicalTrials.gov、ClinicalKey、Cochrane CENTRAL和Web of Science进行电子检索后应用该模型。主要结局为发热持续时间缩短/发热消退严重程度减轻。KD的初始阶段定义为治疗KD患者的第一阶段;KD的难治阶段指对标准KD治疗无反应的KD患者。静脉注射免疫球蛋白(IVIG)的截断点为低剂量(100 - 400mg)、中剂量(1g)和高剂量(至少2g)。
共纳入56项RCT,6486名参与者。NMA表明,与高剂量IVIG +阿司匹林相比,中剂量IVIG +阿司匹林+英夫利昔单抗[平均差=-1.76天(95%置信区间(95%CI):-3.65至0.13天)]发热持续时间最短;同样,在KD初始阶段,与高剂量IVIG +阿司匹林相比,中剂量IVIG +阿司匹林+英夫利昔单抗[比值比(OR)=0.50,95%CI:0.18 - 1.37]冠状动脉病变(CAL)发生率最低。在KD难治阶段,高剂量IVIG +脉冲类固醇疗法(与仅高剂量IVIG相比,OR = 0.04,95%CI:0.00 - 0.43)发热下降率最佳;同样,与仅高剂量IVIG相比,高剂量IVIG +环孢素[OR = 0.05(95%CI:0.00 - 1.21)]CAL发生率最低。在KD难治阶段,与仅高剂量IVIG组相比,英夫利昔单抗显著提高了缓解率(OR = 0.20,95%CI:0.07 - 0.62)。
NMA表明,IVIG和阿司匹林标准疗法的联合治疗可能对缩短急性KD患者的发热持续时间和降低CAL发生率有额外作用。此外,高剂量IVIG与脉冲类固醇疗法或环孢素疗法的联合治疗可能对提高难治性KD儿童的发热下降率和降低CAL发生率有额外作用。由于本NMA的一些结果应被视为产生假设而非确定性结果,因此需要来自全新随机试验的进一步证据来支持我们的结果。
无。