Habte Aklilu, Wondimu Merertu, Abdulkadir Hanan
School of Public Health, College of Medicine and Health Sciences, Wachemo University, Hosaena, Ethiopia.
School of nursing and midwifery, Faculty of health science, Institute of Health, Jimma University, Southwest, Jimma, Ethiopia.
Arch Public Health. 2022 Mar 23;80(1):89. doi: 10.1186/s13690-022-00859-6.
Pieces of evidence strongly indicate that providing high-quality family planning services is accompanied by an increase in contraceptive uptake and a decrease in contraception discontinuation. Contraceptive, especially Implanon discontinuation is a global issue that could be linked to a summary outcome indicator of poor family planning service quality. Although Implanon is becoming more popular among Ethiopian contraceptive users, little is known regarding the survival and predictors of discontinuation. The study aimed at exploring the survival and predictors of Implanon discontinuation among women enrolled in family planning units of Public hospitals in southern Ethiopia, 2021.
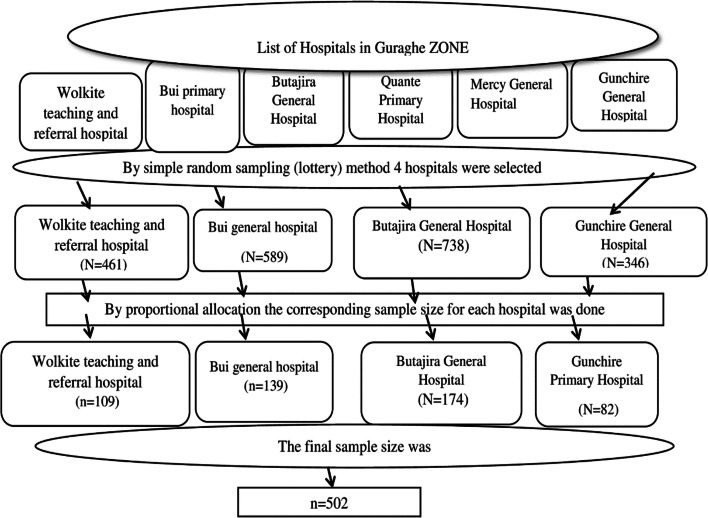
A hospital-based retrospective cohort study was conducted among Implanon users who enrolled in family planning units of Public Hospitals. Five years of medical records, from January 1, 2016, to December 30, 2020, were reviewed. A total of 502 women were selected by using a random sampling technique. A standardized abstraction tool was used to collect data from medical records and registration books. The data were entered into Epidata Version 3.1 and then exported to STATA 14 for analysis. The median was calculated in the case of survival time. Across covariates, the Kaplan Meier survival curve was used to estimate time to Implanon discontinuation. To identify statistically significant predictors of Implanon discontinuation, a multivariable Cox proportional hazard model was fitted.
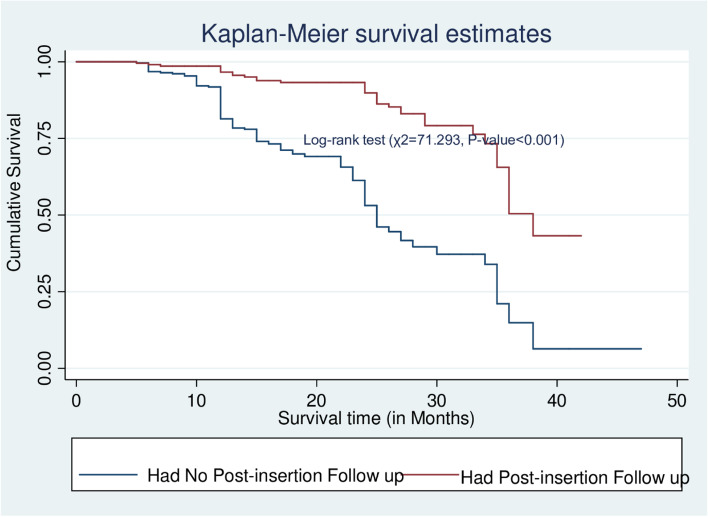
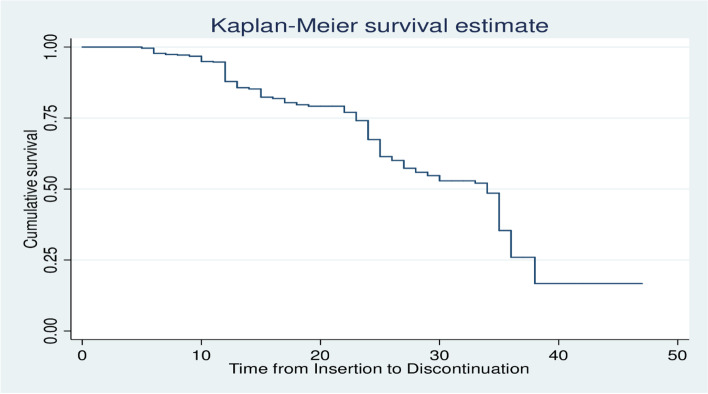
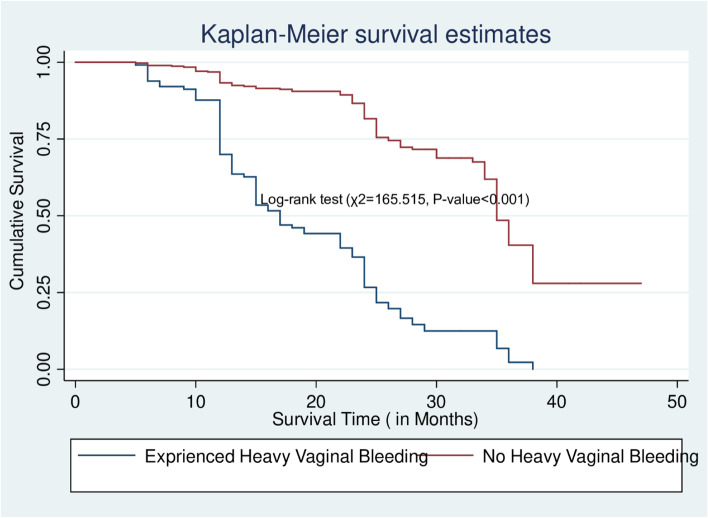
The incidence rate of Implanon discontinuation was 1.87(95% CI = 1.63, 2.15) per 100 person-months of observation. The overall estimated survival probability at the end of 24 and 36 months was 67.4% (95%CI, 62.5, 71.8) and 25.9% (95%CI, 18.4, 34.1) months respectively. Residence [AHR = 1.50; 95%CI: 1.09, 2.08], parity [AHR = 2.02; 95%CI: 1.65, 3.67], pre-insertion counselling [AHR = 2.41; 95%CI: 1.72, 3.70], experiencing heavy vaginal bleeding [AHR = 3.91; 95%CI: 2.67, 5.32], post-insertion follow up [AHR = 3.15; 95%CI:2.11, 4.75] were identified as a significant predictors of Implanon discontinuation.
The risk Implanon of discontinuation was high, especially at 24 and 36 months. In family planning service delivery points, health care providers should pay special attention to clients who live in rural areas and do not have children. In addition, health care providers should provide pre-insertion counseling and post-insertion follow-up that focus on potential side effects. Finally, family planning units need to engage in early side effect management and reassurance to mitigate discontinuation.
大量证据有力表明,提供高质量的计划生育服务会使避孕药具的使用增加,避孕措施的中断减少。避孕措施,尤其是依伴侬(Implanon)的停用是一个全球性问题,这可能与计划生育服务质量差的总体结果指标相关。尽管依伴侬在埃塞俄比亚避孕药具使用者中越来越受欢迎,但关于其停用的留存率和预测因素却知之甚少。本研究旨在探讨2021年埃塞俄比亚南部公立医院计划生育部门登记的女性中依伴侬停用的留存率和预测因素。
对公立医院计划生育部门登记的依伴侬使用者进行了一项基于医院的回顾性队列研究。回顾了2016年1月1日至2020年12月30日的五年医疗记录。采用随机抽样技术共选取了502名女性。使用标准化的摘要工具从医疗记录和登记簿中收集数据。数据录入Epidata 3.1版本,然后导出到STATA 14进行分析。生存时间采用中位数计算。通过协变量,使用Kaplan Meier生存曲线估计依伴侬停用时间。为了确定依伴侬停用的统计学显著预测因素,拟合了多变量Cox比例风险模型。
依伴侬停用的发生率为每100人月观察期1.87(95%CI = 1.63,2.15)。在24个月和36个月结束时,总体估计生存概率分别为67.4%(95%CI,62.5,71.8)和25.9%(95%CI,18.4,34.1)。居住地[AHR = 1.50;95%CI:1.09,2.08]、产次[AHR = 2.02;95%CI:1.65,3.67]、植入前咨询[AHR = 2.41;95%CI:1.72,3.70]、经历大量阴道出血[AHR = 3.91;95%CI:2.67,5.32]、植入后随访[AHR = 3.15;95%CI:2.11,4.75]被确定为依伴侬停用的显著预测因素。
依伴侬停用的风险很高,尤其是在24个月和36个月时。在计划生育服务提供点,医疗保健提供者应特别关注居住在农村地区且没有孩子的客户。此外,医疗保健提供者应提供侧重于潜在副作用的植入前咨询和植入后随访。最后,计划生育部门需要尽早进行副作用管理并给予安心措施以减少停用。