Department of Surgery, University of Arizona College of Medicine, Tucson.
Southwestern Academic Limb Salvage Alliance (SALSA), Los Angeles, California.
JAMA Netw Open. 2022 Mar 1;5(3):e223991. doi: 10.1001/jamanetworkopen.2022.3991.
It is not known whether implementation of Medicaid expansion under the Patient Protection and Affordable Care Act (ACA) was associated with improvements in the outcomes among racial and ethnic minority adults at risk of diabetes-related major amputations.
To explore the association of early Medicaid expansion with outcomes of diabetic foot ulcerations (DFUs).
DESIGN, SETTING, AND PARTICIPANTS: This cohort study included hospitalizations for DFUs among African American, Asian and Pacific Islander, American Indian or Alaska Native, and Hispanic adults as well as adults with another minority racial or ethnic identification aged 20 to 64 years. Data were collected from the State Inpatient Databases for 19 states and the District of Columbia for 2013 to the third quarter of 2015. The analysis was performed on December 4, 2019, and updated on November 9, 2021.
States were categorized into early-adopter states (expansion by January 2014) and nonadopter states.
Poisson regression was performed to examine the associations of state type, time, and their combined association with the proportional changes of major amputation rate per year per 100 000 population.
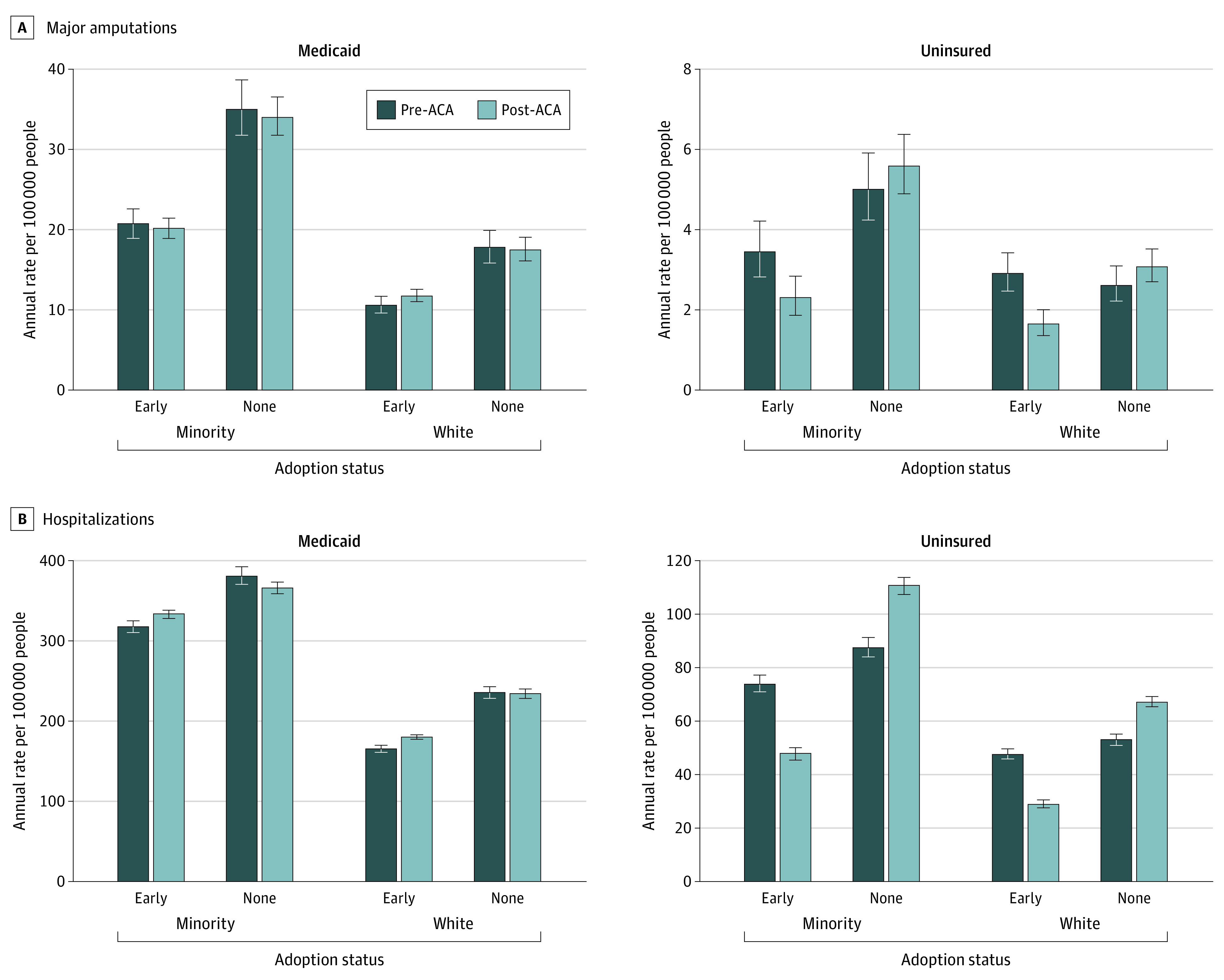
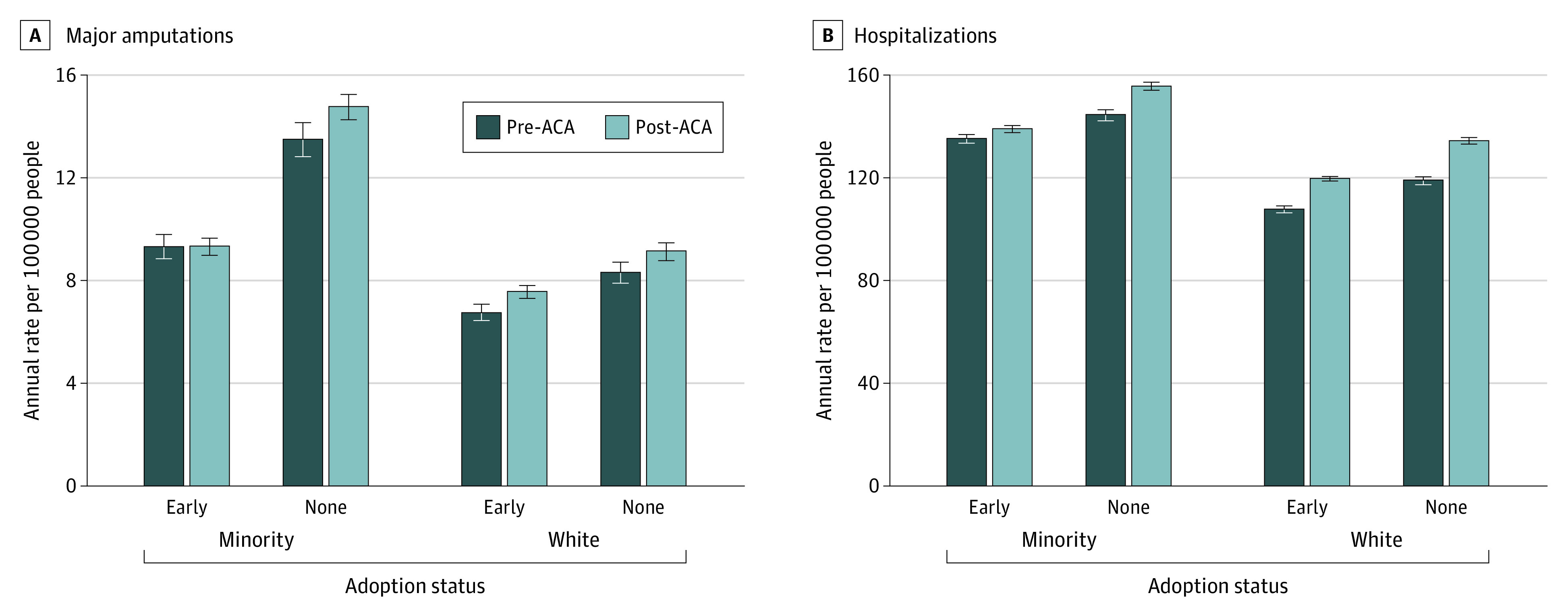
Among the 115 071 hospitalizations among racial and ethnic minority adults with DFUs (64% of sample aged 50 to 64 years; 35%, female; 61%, African American; 25%, Hispanic; 14%, other racial and ethnic minority group), there were 36 829 hospitalizations (32%) for Medicaid beneficiaries and 10 500 hospitalizations (9%) for uninsured patients. Hospitalizations increased 3% (95% CI, 1% to 5%) in early-adopter states and increased 8% (95% CI, 6% to 10%) in nonadopter states after expansion, a significant difference (P for interaction < .001). Although there was no change in the amputation rate (0.08%; 95% CI, -6% to 7%) in early-adopter states after expansion, there was a 9% (95% CI, 3% to 16%) increase in nonadopter states, a significant change (P = .04). For uninsured adults, the amputation rate decreased 33% (95% CI, 10% to 50%) in early-adopter states and did not change (12%; 95% CI, -10% to 38%) in nonadopter states after expansion, a significant difference (P = .006). There was no difference in the change of amputation rate among Medicaid beneficiaries between state types after expansion.
This study found a relative improvement in the major amputation rate among African American, Hispanic, and other racial and ethnic minority adults in early-expansion states compared with nonexpansion states, which could be because of the recruitment of at-risk uninsured adults into the Medicaid program during the first 2 years of ACA implementation. Future study is required to evaluate the long-term association of Medicaid expansion and the rates of amputation.
重要性:尚不清楚《平价医疗法案》(ACA)实施医疗补助计划扩大范围是否与糖尿病相关主要截肢风险的少数民族成年人的结局改善有关。
目的:探讨早期医疗补助计划扩大范围与糖尿病足溃疡(DFU)结局的关系。
设计、地点和参与者:本队列研究纳入了年龄在 20 至 64 岁之间的非裔美国人、亚洲和太平洋岛民、美国印第安人或阿拉斯加原住民以及西班牙裔成年人以及其他少数民族种族或族裔身份的成年人因 DFU 住院的情况。数据来自 19 个州和哥伦比亚特区的州住院患者数据库,时间范围为 2013 年至 2015 年第三季度。分析于 2019 年 12 月 4 日进行,并于 2021 年 11 月 9 日更新。
暴露情况:根据各州是否为早期采用州(在 2014 年 1 月之前扩大)进行分类。
主要结果和测量:采用泊松回归分析研究州类型、时间及其综合关联与每 10 万人每年主要截肢率的比例变化之间的关系。
结果:在 115071 名有 DFU 的少数民族成年人住院患者中(64%的样本年龄在 50 至 64 岁之间;35%为女性;61%为非裔美国人;25%为西班牙裔;14%为其他少数民族群体),有 36829 名(32%)为医疗补助受助人,10500 名(9%)为无保险患者。在扩张后的早期采用州,住院人数增加了 3%(95%CI,1%至 5%),而在非采用州,住院人数增加了 8%(95%CI,6%至 10%),差异显著(P<0.001)。虽然扩张后早期采用州的截肢率没有变化(0.08%;95%CI,-6%至 7%),但非采用州的截肢率增加了 9%(95%CI,3%至 16%),这是一个显著变化(P=0.04)。对于无保险成年人,在早期采用州,截肢率下降了 33%(95%CI,10%至 50%),而在非采用州,截肢率没有变化(12%;95%CI,-10%至 38%),差异显著(P=0.006)。扩张后,州类型之间医疗补助受益人的截肢率变化没有差异。
结论和相关性:本研究发现,与非扩张州相比,在早期扩张州,非裔美国人、西班牙裔和其他少数民族成年人的主要截肢率有所改善,这可能是因为在 ACA 实施的头两年,有风险的无保险成年人被纳入了医疗补助计划。需要进一步研究来评估医疗补助计划扩大范围与截肢率的长期关联。