Jenkins R L, Clowes G H, Bosari S, Pearl R H, Khettry U, Trey C
Ann Surg. 1986 Oct;204(4):364-74. doi: 10.1097/00000658-198610000-00004.
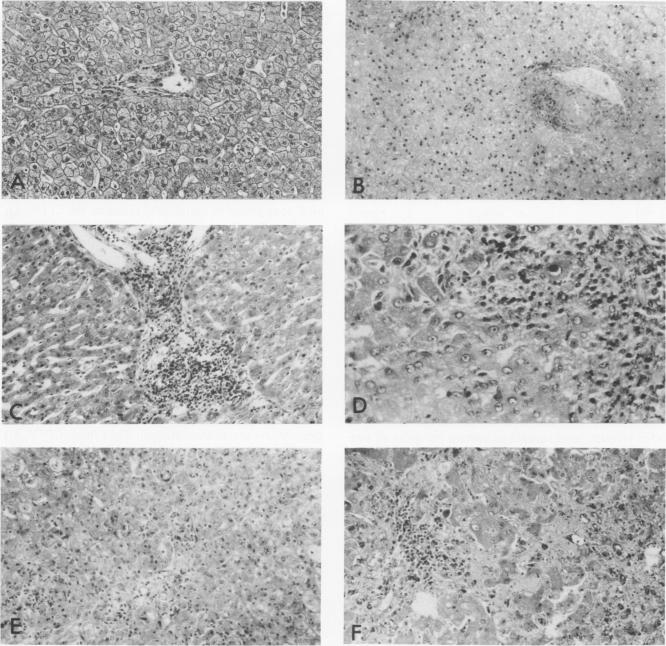
Forty-one patients, all in end stage hepatic failure, underwent 46 liver transplantations with a long-term survival rate of 63%. Six patients died of uncontrollable bleeding due to primary graft malfunction at or immediately after operation. Nine died early or late with overwhelming infection. In addition to clinical assessment, needle liver biopsy, central plasma clearance rate of amino acids (CPCR-AA), and routine "liver function tests" were employed to aid in selection of patients for transplantation and for guidance in postoperative management. Although liver biopsies usually afforded an exact diagnosis, neither they nor the routine liver function tests quantitated the extent to which hepatocyte function was impaired. CPCR-AA, which measures the rate of amino acid uptake by the liver and other central tissues for oxidation, gluconeogenesis, and protein synthesis was 91 +/- 9 ml/M2/min in the preoperative transplant group. This compares with a value of 97 +/- 16 in a previously studied series of cirrhotics who died following other forms of surgery and a CPCR-AA of 220 +/- 26 ml/m2/min in those who survived. In addition, the preoperative CPCR-AA was found to correlate with the in vitro hepatic protein synthetic rate of slices from the resected recipient liver (r = 0.72, p less than 0.02). After operation, serial hepatic needle biopsies were classified by histology into four grades of injury, ranging from normal liver transplant (Grade I) to mild hypoxic or rejection injury (Grade II), viral hepatitis (Grade III), and severe hypoxic or rejection injury (Grade IV). Significant relationships of the histological grades to ultimate mortality, CPCR-AA, and prothrombin times were found. CPCR-AA and prothrombin time correlate inversely (r = 0.57, p less than 0.001), further demonstrating the relationship of CPCR-AA to protein synthesis of clotting factors. These patterns of posttransplant response were delineated by serial CPCR-AA values. "Early" responders had values over 290 ml/M2/min and all survived. Twelve patients with delayed response were characterized by values of 150 +/- 12, rising to over 200 ml/M2/min after 2 weeks. Two who failed to increase CPCR-AA died. In six "poor" responders, CPCR-AA with Grade IV injury remained below 110 ml/M2/min. All died except for one whose CPCR-AA subsequently rose following retransplantation. It is concluded that percutaneous hepatic needle biopsies and CPCR-AA measurements in combination are of proven value, not only in understanding the nature of injury and functional impairment of the liver, but are also important as guides to selection of patients and for their posttransplant management.
41例均处于终末期肝衰竭的患者接受了46次肝移植,长期生存率为63%。6例患者因原发性移植物功能障碍在手术中或术后即刻死于无法控制的出血。9例患者因严重感染于术后早期或晚期死亡。除了临床评估外,还采用经皮肝穿刺活检、肝脏氨基酸中央血浆清除率(CPCR - AA)和常规“肝功能检查”来辅助选择移植患者并指导术后管理。尽管肝穿刺活检通常能做出准确诊断,但无论是肝穿刺活检还是常规肝功能检查都无法定量肝细胞功能受损的程度。CPCR - AA测量肝脏及其他中央组织摄取氨基酸用于氧化、糖异生和蛋白质合成的速率,术前移植组该值为91±9 ml/M2/min。与之相比,先前研究的一系列因其他形式手术死亡的肝硬化患者该值为97±16,而存活患者的CPCR - AA为220±26 ml/m2/min。此外,发现术前CPCR - AA与切除的受者肝脏切片的体外肝蛋白合成速率相关(r = 0.72,p < 0.02)。术后,系列肝穿刺活检经组织学分类为4级损伤,从正常肝移植(I级)到轻度缺氧或排斥损伤(II级)、病毒性肝炎(III级)和严重缺氧或排斥损伤(IV级)。发现组织学分级与最终死亡率、CPCR - AA和凝血酶原时间之间存在显著相关性。CPCR - AA与凝血酶原时间呈负相关(r = 0.57,p < 0.001),进一步证明了CPCR - AA与凝血因子蛋白合成之间的关系。这些移植后反应模式通过系列CPCR - AA值得以描绘。“早期”反应者的值超过290 ml/M2/min且全部存活。12例反应延迟的患者其值为150±12,2周后升至超过200 ml/M2/min。2例CPCR - AA未升高的患者死亡。6例“反应不佳”的患者中,IV级损伤时CPCR - AA仍低于每平方米每分钟110毫升。除1例在再次移植后CPCR - AA随后升高的患者外,其余全部死亡。结论是经皮肝穿刺活检和CPCR - AA测量相结合不仅在了解肝脏损伤性质和功能损害方面已被证明有价值,而且在指导患者选择及其移植后管理方面也很重要。