Section of General Internal Medicine, Department of Internal Medicine, Yale School of Medicine, New Haven, Connecticut.
Cancer Outcomes, Public Policy, and Effectiveness Research Center, Yale Cancer Center and Yale University School of Medicine, New Haven, Connecticut.
JAMA Netw Open. 2022 Mar 1;5(3):e224208. doi: 10.1001/jamanetworkopen.2022.4208.
Digital breast tomosynthesis (DBT) is a breast cancer screening modality that has gained popularity in recent years. Although insurance coverage for DBT is not mandated under the Patient Protection and Affordable Care Act, several states have required coverage without cost sharing for private insurers.
To evaluate the association between state-level insurance coverage mandates for DBT and changes in DBT use, price, and out-of-pocket payments.
DESIGN, SETTING, AND PARTICIPANTS: This cohort study used an event-study design with repeated cross-sectional observations of US states. Data were obtained from the Blue Cross Blue Shield Axis database for commercially insured women aged 40 to 64 years who underwent screening mammography between January 1, 2015, and June 30, 2019. Data were analyzed between January 14, 2021, and January 20, 2022.
Passage of state-level legislation requiring insurance coverage of DBT.
Change in DBT use among women screened for breast cancer, overall DBT price, and out-of-pocket payments for DBT in states with mandates for coverage of DBT compared with states that did not pass legislation.
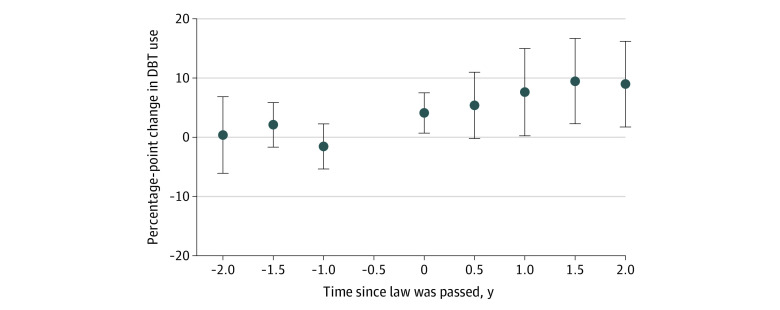
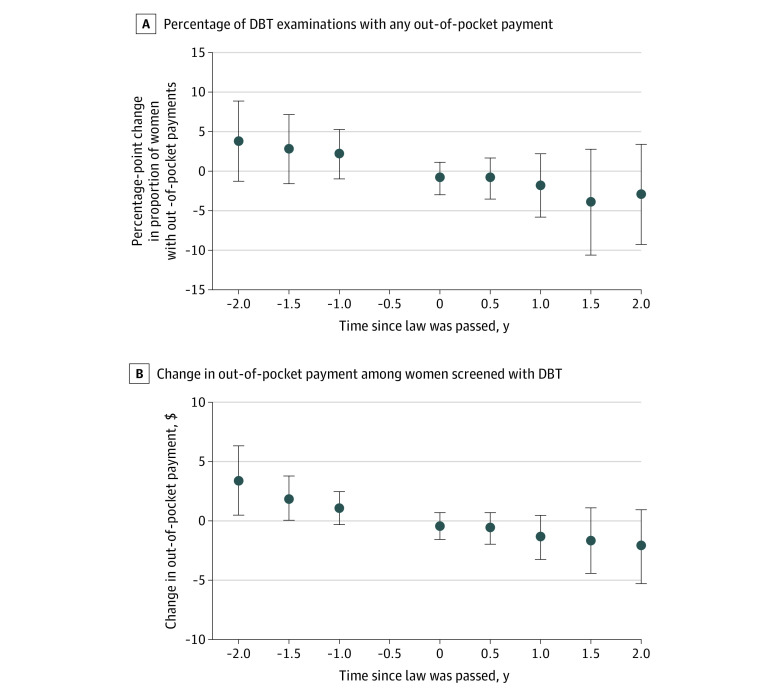
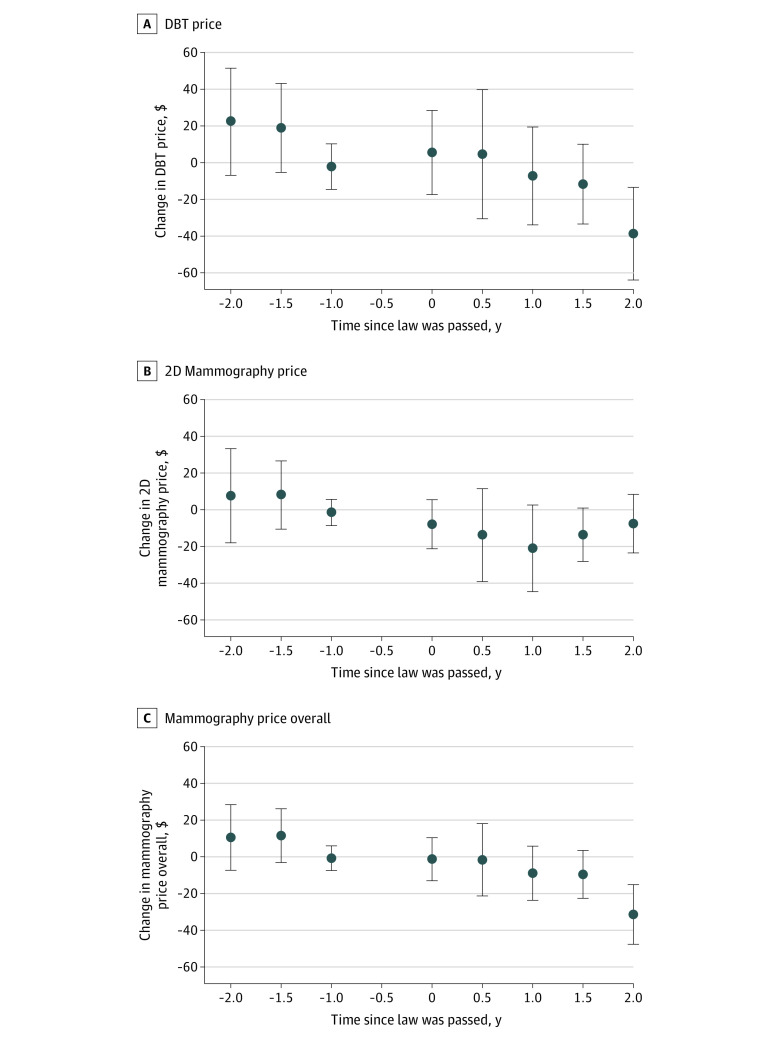
This study included 9 604 084 screening mammograms from 5 754 123 women (mean [SD] age, of 53 [6.7] years). During the study period, 15 states enacted DBT coverage mandates and 34 states did not. In states with coverage mandates, DBT use increased by 9.0 percentage points (95% CI, 1.8-16.3 percentage points; P = .02) 2 years after the mandate compared with states without coverage mandates. Coverage mandates were also associated with a net $38.7 (95% CI, $13.4-$63.9; P = .003) decrease in the mean price of DBT compared with no coverage mandates. There was no association between coverage mandates and out-of-pocket payments 2 years after mandate passage ($-2.1; 95% CI, $-5.3 to $1.0; P = .18).
In this cohort study, DBT coverage mandates were associated with an increase in DBT use but not with any change in out-of-pocket payments. The findings suggest that coverage mandates for DBT may have been associated with broader use but were not associated with changes in direct costs to patients.
数字乳腺断层摄影术(DBT)是一种近年来越来越受欢迎的乳腺癌筛查方式。尽管《患者保护与平价医疗法案》并未强制要求为 DBT 提供保险,但一些州已经要求私人保险公司对其进行无共同支付的覆盖。
评估州级 DBT 保险覆盖范围的规定与 DBT 使用、价格和自付费用变化之间的关系。
设计、设置和参与者:本队列研究采用事件研究设计,对美国各州进行了重复的横断面观察。数据来自 Blue Cross Blue Shield Axis 数据库,包括 2015 年 1 月 1 日至 2019 年 6 月 30 日期间接受筛查性乳房 X 光检查的 40 至 64 岁商业保险女性。数据分析于 2021 年 1 月 14 日至 2022 年 1 月 20 日进行。
州立法通过,要求保险涵盖 DBT。
与没有通过立法的州相比,在有 DBT 覆盖范围规定的州中,筛查乳腺癌的女性中 DBT 使用的变化、总体 DBT 价格和 DBT 的自付费用。
本研究包括了 5754123 名女性的 9604084 次筛查性乳房 X 光检查(平均[标准差]年龄,53[6.7]岁)。在研究期间,有 15 个州颁布了 DBT 覆盖法规,而 34 个州没有。在有覆盖范围的州,DBT 的使用率在法规颁布后 2 年增加了 9.0 个百分点(95%置信区间,1.8-16.3 个百分点;P = .02),而没有覆盖范围的州则没有。覆盖范围的规定还与 DBT 的平均价格净降低 38.7 美元(95%置信区间,13.4-63.9 美元;P = .003)相关,而没有覆盖范围的州则没有。在法规颁布后 2 年,覆盖范围的规定与自付费用之间没有关联(-2.1 美元;95%置信区间,-5.3 至 1.0 美元;P = .18)。
在这项队列研究中,DBT 覆盖范围的规定与 DBT 使用的增加有关,但与患者的自付费用变化无关。这些发现表明,DBT 的覆盖范围规定可能与更广泛的使用有关,但与患者直接费用的变化无关。