Yang Joe, Naik Jaesh, Massello Matthew, Ralph Lewis, Dillon Ryan James
Merck & Co., Inc., Kenilworth, NJ, USA.
BresMed Health Solutions Ltd, Sheffield, UK.
Infect Dis Ther. 2022 Aug;11(4):1443-1457. doi: 10.1007/s40121-022-00607-x. Epub 2022 Mar 25.
Imipenem/cilastatin/relebactam (IMI/REL), a combination β-lactam antibiotic (imipenem) with a novel β-lactamase inhibitor (relebactam), is an efficacious and well-tolerated option for the treatment of hospitalized patients with gram-negative (GN) bacterial infections caused by carbapenem-non-susceptible (CNS) pathogens. This study examines cost-effectiveness of IMI/REL vs. colistin plus imipenem (CMS + IMI) for the treatment of infection(s) caused by confirmed CNS pathogens.
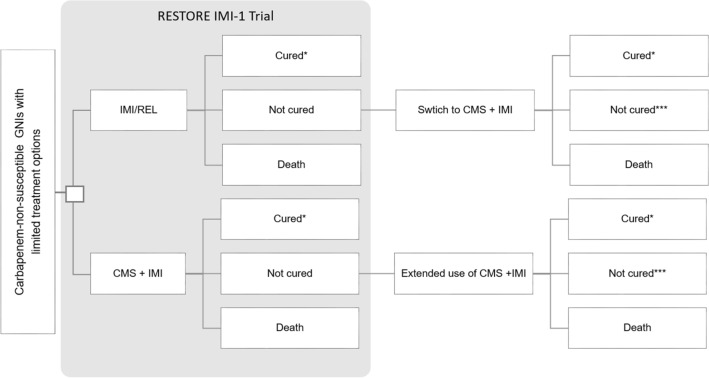
We developed an economic model comprised of a decision-tree depicting initial hospitalization, and a Markov model projecting long-term health and economic impacts following discharge. The decision tree, informed by clinical data from RESTORE-IMI 1 trial, modeled clinical outcomes (mortality, cure rate, and adverse events including nephrotoxicity) in the two comparison scenarios of IMI/REL versus CMS + IMI for patients with CNS GN infection. Subsequently, a Markov model translated these hospitalization stage outcomes (i.e., death or uncured infection) to long-term consequences such as quality-adjusted life years (QALYs). Sensitivity analyses were conducted to test the model robustness.
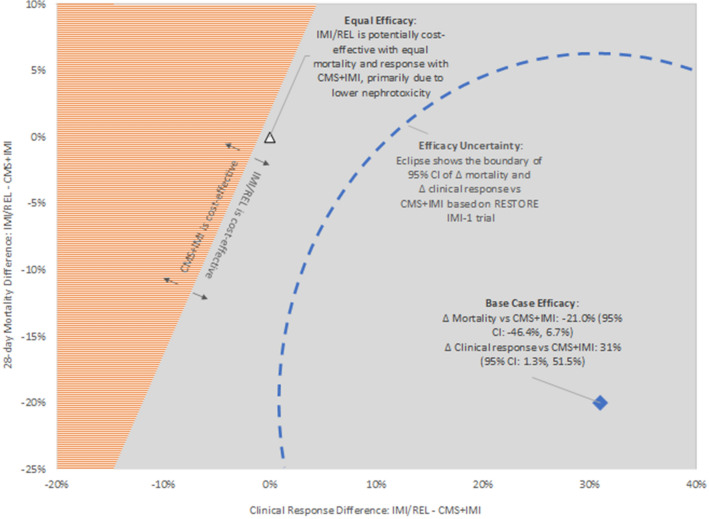
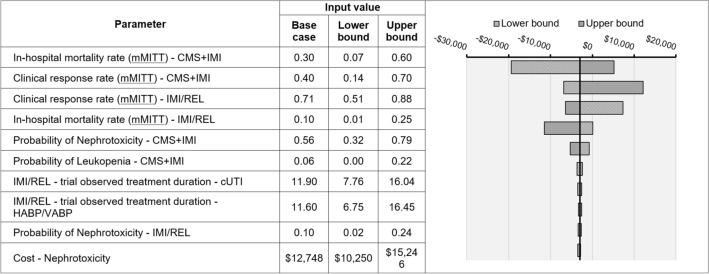
IMI/REL compared to CMS + IMI demonstrated a higher cure rate (79.0% vs. 52.0%), lower mortality (15.2% vs. 39.0%), and reduced nephrotoxicity (14.6% vs. 56.4%). On average a patient treated with IMI/REL vs. CMS + IMI gained additional 3.7 QALYs over a lifetime. Higher drug acquisition costs for IMI/REL were offset by shorter hospital length of stay and lower AE-related costs, which result in net savings of $11,015 per patient. Sensitivity analyses suggested that IMI/REL has a high likelihood (greater than 95%) of being cost-effective at a US willingness-to-pay threshold of $100,000-150,000 per QALY.
For patients with confirmed CNS GN infection, IMI/REL could yield favorable clinical outcomes and may be cost-saving-as the higher IMI/REL drug acquisition cost is offset by reduced nephrotoxicity-related cost-for the US payer compared to CMS + IMI.
亚胺培南/西司他丁/雷利巴坦(IMI/REL)是一种β-内酰胺类抗生素(亚胺培南)与新型β-内酰胺酶抑制剂(雷利巴坦)的组合,是治疗由碳青霉烯不敏感(CNS)病原体引起的革兰氏阴性(GN)菌感染住院患者的一种有效且耐受性良好的选择。本研究考察了IMI/REL与黏菌素加亚胺培南(CMS + IMI)治疗确诊为CNS病原体所致感染的成本效益。
我们构建了一个经济模型,包括一个描述初始住院情况的决策树,以及一个预测出院后长期健康和经济影响的马尔可夫模型。该决策树以RESTORE-IMI 1试验的临床数据为依据,对IMI/REL与CMS + IMI两种比较方案中CNS GN感染患者的临床结局(死亡率、治愈率以及包括肾毒性在内的不良事件)进行建模。随后,马尔可夫模型将这些住院阶段的结局(即死亡或未治愈的感染)转化为长期后果,如质量调整生命年(QALY)。进行敏感性分析以检验模型的稳健性。
与CMS + IMI相比,IMI/REL显示出更高的治愈率(79.0%对52.0%)、更低的死亡率(15.2%对39.0%)以及更低的肾毒性(14.6%对56.4%)。平均而言,接受IMI/REL治疗的患者比接受CMS + IMI治疗的患者一生可多获得3.7个QALY。IMI/REL较高的药品采购成本被较短的住院时间和较低的与不良事件相关的成本所抵消,从而使每位患者节省净费用11,015美元。敏感性分析表明,在美国每QALY支付意愿阈值为100,000 - 150,000美元时,IMI/REL具有较高的成本效益可能性(大于95%)。
对于确诊为CNS GN感染的患者,与CMS + IMI相比,IMI/REL可产生良好的临床结局,并且可能节省成本——因为IMI/REL较高的药品采购成本被降低的肾毒性相关成本所抵消——对于美国支付方而言。