Disease Control Department, London School of Hygiene & Tropical Medicine, London, UK
Institute for Global Health, University College London, London, UK.
BMJ Glob Health. 2024 Feb 29;9(2):e013205. doi: 10.1136/bmjgh-2023-013205.
Limited information on costs and the cost-effectiveness of hospital interventions to reduce antibiotic resistance (ABR) hinder efficient resource allocation.
We conducted a systematic literature review for studies evaluating the costs and cost-effectiveness of pharmaceutical and non-pharmaceutical interventions aimed at reducing, monitoring and controlling ABR in patients. Articles published until 12 December 2023 were explored using EconLit, EMBASE and PubMed. We focused on critical or high-priority bacteria, as defined by the WHO, and intervention costs and incremental cost-effectiveness ratio (ICER). Following Preferred Reporting Items for Systematic review and Meta-Analysis guidelines, we extracted unit costs, ICERs and essential study information including country, intervention, bacteria-drug combination, discount rates, type of model and outcomes. Costs were reported in 2022 US dollars ($), adopting the healthcare system perspective. Country willingness-to-pay (WTP) thresholds from Woods 2016 guided cost-effectiveness assessments. We assessed the studies reporting checklist using Drummond's method.
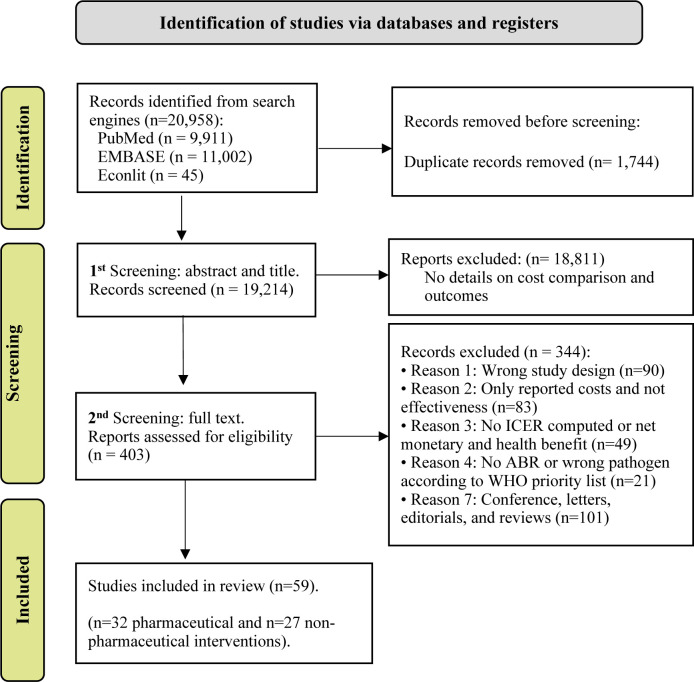
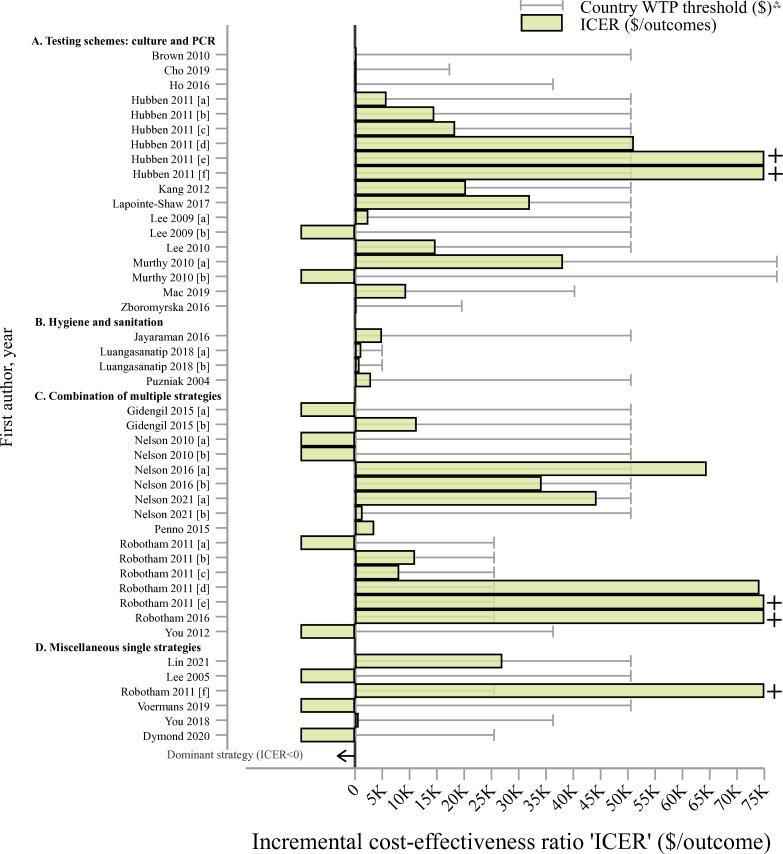
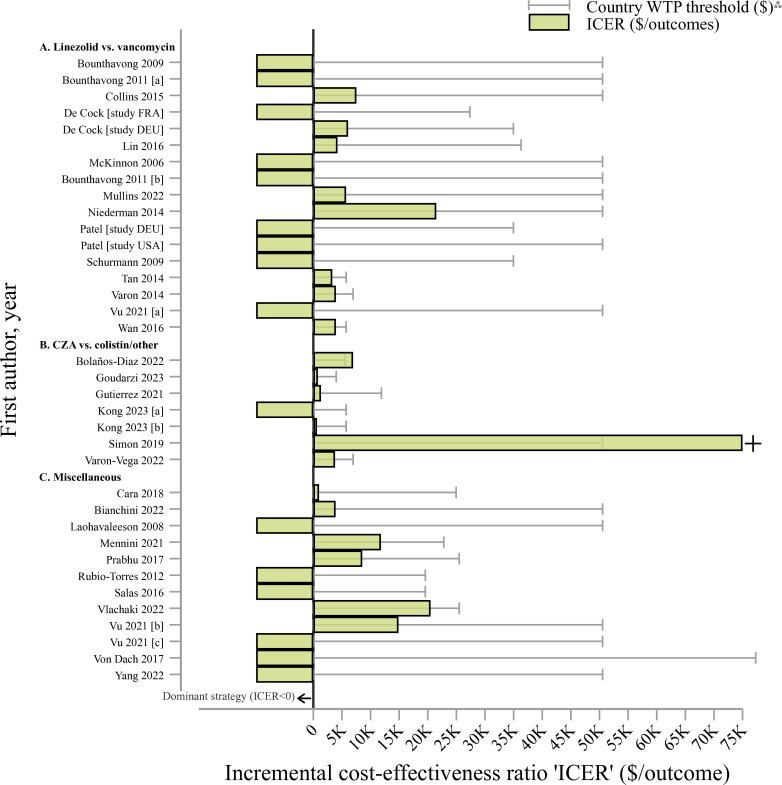
Among 20 958 articles, 59 (32 pharmaceutical and 27 non-pharmaceutical interventions) met the inclusion criteria. Non-pharmaceutical interventions, such as hygiene measures, had unit costs as low as $1 per patient, contrasting with generally higher pharmaceutical intervention costs. Several studies found that linezolid-based treatments for methicillin-resistant were cost-effective compared with vancomycin (ICER up to $21 488 per treatment success, all 16 studies' ICERs<WTP). Infection control measures such as hand hygiene and gown usage (ICER=$1160/QALY or $4949 per ABR case averted, all ICERs<WTP) and PCR or chromogenic agar screening for ABR detection were highly cost-effective (eg, ICER=$1206 and $1115 per life-year saved in Europe and the USA). Comparisons were hindered by within-study differences.
Robust information on ABR interventions is critical for efficient resource allocation. We highlight cost-effective strategies for mitigating ABR in hospitals, emphasising substantial knowledge gaps, especially in low-income and middle-income countries. Our study serves as a resource for guiding future cost-effectiveness study design and analyses. CRD42020341827 and CRD42022340064.
医院干预措施降低抗生素耐药性(ABR)的成本和成本效益信息有限,阻碍了资源的有效分配。
我们对评估旨在减少、监测和控制患者 ABR 的药物和非药物干预措施的成本和成本效益的研究进行了系统文献回顾。使用 EconLit、EMBASE 和 PubMed 检索了截至 2023 年 12 月 12 日发表的文章。我们关注世界卫生组织(WHO)定义的关键或高优先级细菌,以及干预措施成本和增量成本效益比(ICER)。我们遵循系统评价和荟萃分析指南的首选报告项目,提取单位成本、ICER 和基本研究信息,包括国家、干预措施、细菌-药物组合、折扣率、模型类型和结果。采用卫生保健系统视角,以 2022 年美元($)报告成本。Woods 2016 年的国家意愿支付(WTP)阈值指导成本效益评估。我们使用 Drummond 方法评估报告清单的研究。
在 20958 篇文章中,有 59 篇(32 项药物干预和 27 项非药物干预)符合纳入标准。非药物干预措施,如卫生措施,每个患者的单位成本低至 1 美元,而药物干预措施的成本通常较高。几项研究发现,利奈唑胺治疗耐甲氧西林金黄色葡萄球菌的成本效益优于万古霉素(治疗成功率的 ICER 高达 21488 美元/例,所有 16 项研究的 ICER<WTP)。感染控制措施,如手部卫生和穿手术服(ICER=$1160/QALY 或每例 ABR 病例避免的费用为$4949,所有 ICER<WTP)和聚合酶链反应或显色琼脂筛查 ABR 检测非常具有成本效益(例如,在欧洲和美国,每挽救一个生命年的 ICER 分别为$1206 和$1115)。由于研究内差异,比较受到阻碍。
有关 ABR 干预措施的可靠信息对于资源的有效分配至关重要。我们强调了在医院减轻 ABR 的具有成本效益的策略,强调了特别是在低收入和中等收入国家存在重大知识差距。我们的研究为指导未来的成本效益研究设计和分析提供了资源。CRD42020341827 和 CRD42022340064。