From the Department of Psychiatry (A.M., Z.I.), Hotchkiss Brain Institute (A.M., S.N., M.G., S.G., E.S., Z.I.), Mathison Centre for Mental Health Research and Education (A.M., Z.I.), Department of Clinical Neurosciences (E.S., Z.I.), Department of Community Health Sciences (Z.I.), and O'Brien Institute for Public Health (Z.I.), Cumming School of Medicine, University of Calgary, Alberta, Canada.
Neurology. 2022 May 24;98(21):e2132-e2139. doi: 10.1212/WNL.0000000000200256. Epub 2022 Mar 29.
Mild cognitive impairment (MCI) is an at-risk state for dementia; however, not all individuals with MCI transition to dementia, and some revert to normal cognition (NC). Here, we investigate whether mild behavioral impairment (MBI), the late-life onset of persistent neuropsychiatric symptoms (NPS), improves the prognostic specificity of MCI.
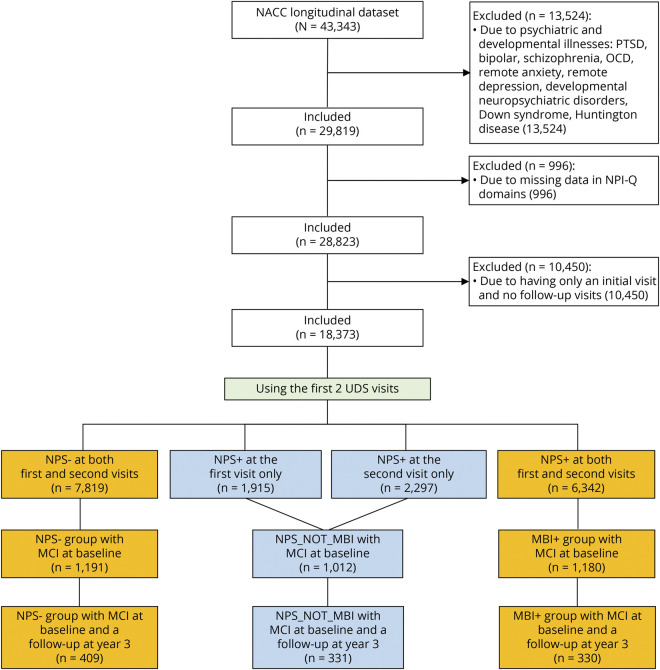
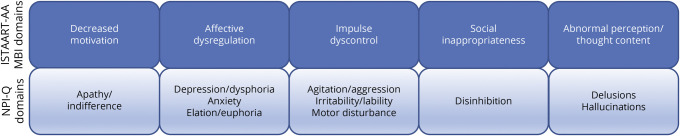
Participants with MCI from the National Alzheimer's Coordinating Center Uniform Data Set were included. NPS were operationalized with the Neuropsychiatric Inventory Questionnaire to identify participants without NPS and those with MBI (persistent, late-onset NPS). Individuals with late-onset NPS not meeting the MBI persistence criterion (NPS_NOT_MBI) were retained for secondary analyses. Progression to dementia, stable MCI, and reversion to NC after 3 years of follow-up were defined per National Institute on Aging-Alzheimer's Association and Petersen criteria.
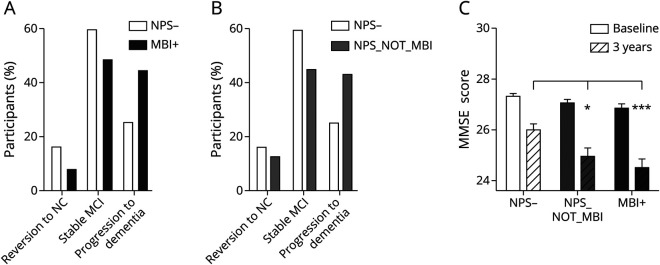
The primary sample consisted of 739 participants (NPS- n = 409 and MBI+ n = 330; 75.16 ± 8.6 years old, 40.5% female). After 3 years, 238 participants (33.6%) progressed to dementia, and 90 (12.2%) reverted to NC. Compared to participants without NPS, participants with MBI were significantly more likely to progress to dementia (adjusted odds ratio [AOR] 2.13, 95% CI 1.52-2.99), with an annual progression rate of 14.7% (vs 8.3% for participants with MCI without NPS). Compared to participants without NPS, participants with MBI were less likely to revert to NC (AOR 0.48, 95% CI 0.28-0.83, 2.5% vs 5.3% annual reversion rate). The NPS_NOT_MBI group (n = 331, 76.5 ± 8.6 years old, 45.9% female) were more likely to progress to dementia (AOR 2.18, 95% CI 1.56-3.03, 14.3% annual progression rate) but not less likely to revert to NC than those without NPS. Accordingly, both NPS_NOT_MBI and MBI+ participants had lower Mini-Mental State Examination scores than NPS- participants after 3 years.
Late-onset NPS improve the specificity of MCI as an at-risk state for progression to dementia. However, only persistent late-onset NPS are associated with a lower likelihood of reversion to NC, with transient NPS (i.e., NPS_NOT_MBI) not differing from the NPS- group. Clinical prognostication can be improved by incorporating late-onset NPS, especially those that persist (i.e., MBI), into risk assessments. Clinical trials may benefit from enrichment with these higher-risk participants with MCI.
轻度认知障碍(MCI)是痴呆的高危状态;然而,并非所有 MCI 患者都会发展为痴呆,有些患者会恢复正常认知(NC)。在这里,我们研究轻度行为障碍(MBI),即晚年持续性神经精神症状(NPS)的出现,是否能提高 MCI 的预后特异性。
本研究纳入了来自国家阿尔茨海默病协调中心统一数据集的 MCI 患者。使用神经精神问卷(Neuropsychiatric Inventory Questionnaire)来确定有无 NPS,并将 NPS 定义为 MBI(持续性、晚年发生的 NPS)。对于不符合 MBI 持续性标准的晚年发生 NPS 个体(NPS_NOT_MBI),进行了次要分析。根据国家老龄化研究所-阿尔茨海默病协会和彼得森标准,将随访 3 年后进展为痴呆、稳定的 MCI 和恢复为 NC 定义为进展、稳定和恢复。
主要样本包括 739 名参与者(NPS- n = 409,MBI+ n = 330;年龄 75.16 ± 8.6 岁,40.5%为女性)。3 年后,238 名参与者(33.6%)进展为痴呆,90 名参与者(12.2%)恢复为 NC。与无 NPS 的参与者相比,有 MBI 的参与者更有可能进展为痴呆(调整后的优势比 [AOR] 2.13,95%CI 1.52-2.99),其年进展率为 14.7%(而无 NPS 的 MCI 参与者为 8.3%)。与无 NPS 的参与者相比,有 MBI 的参与者更不可能恢复为 NC(AOR 0.48,95%CI 0.28-0.83,2.5%的年恢复率 vs 5.3%)。NPS_NOT_MBI 组(n = 331,年龄 76.5 ± 8.6 岁,45.9%为女性)更有可能进展为痴呆(AOR 2.18,95%CI 1.56-3.03,年进展率为 14.3%),但恢复为 NC 的可能性并不低于无 NPS 的参与者。因此,与 NPS- 参与者相比,NPS_NOT_MBI 和 MBI+ 参与者在 3 年后的简易精神状态检查评分较低。
晚年发生的 NPS 提高了 MCI 作为向痴呆进展的高危状态的特异性。然而,只有持续性晚年发生的 NPS 与恢复为 NC 的可能性较低相关,而短暂性 NPS(即 NPS_NOT_MBI)与 NPS- 组无差异。通过将晚年发生的 NPS,特别是持续性 NPS(即 MBI)纳入风险评估,可以改善临床预后预测。临床试验可能受益于招募这些 MCI 患者中风险更高的参与者。