From the Covid-19 Response Team, Centers for Disease Control and Prevention (A.M.P., S.M.O., M.W.T., L.D.Z., A.P.C., M.M.P.), the Center for Childhood Infections and Vaccines of Children's Healthcare of Atlanta and the Department of Pediatrics, Emory University School of Medicine (S.K.), and the Division of Critical Care Medicine, Department of Pediatrics, Emory University School of Medicine, Children's Healthcare of Atlanta (K.M.T.) - all in Atlanta; the Department of Anesthesiology, Critical Care, and Pain Medicine, Boston Children's Hospital (M.M.N., A.G.R.), and the Departments of Anaesthesia and Pediatrics, Harvard Medical School (A.G.R.) - both in Boston; the Division of Pediatric Infectious Diseases, Department of Pediatrics, Vanderbilt University Medical Center, Nashville (N.B.H.); the Department of Pediatrics, Baylor College of Medicine, Immunization Project, Texas Children's Hospital, Houston (J.A.B., L.C.S.), and the Department of Pediatrics, Division of Critical Care Medicine, University of Texas Southwestern, Children's Medical Center, Dallas (M.M.); the Division of Infectious Diseases, Children's Hospital Los Angeles and Departments of Pediatrics and Molecular Microbiology and Immunology, University of Southern California, Los Angeles (P.S.P.), the Division of Pediatric Hospital Medicine, UC San Diego-Rady Children's Hospital, San Diego (M.A.C.), the Division of Critical Care Medicine, UCSF Benioff Children's Hospital, Oakland (N.Z.C.), and the Department of Pediatrics, Divisions of Critical Care Medicine and Allergy, Immunology, and Bone Marrow Transplant, University of California, San Francisco, San Francisco (M.S.Z.) - all in California; Section of Pediatric Critical Care, Department of Pediatrics, Arkansas Children's Hospital, Little Rock (K.I.); the Division of Pediatric Critical Care Medicine, Nationwide Children's Hospital Columbus (K.E.B.), the Division of Critical Care Medicine, Department of Pediatrics, Akron Children's Hospital, Akron (R.A.N.), and the Department of Pediatrics, University of Cincinnati College of Medicine, Cincinnati Children's Hospital Medical Center, Cincinnati (M.A.S.) - all in Ohio; the Department of Pediatrics, Section of Critical Care Medicine, University of Colorado School of Medicine and Children's Hospital Colorado, Aurora (A.B.M.); the Department of Pediatrics, University of North Carolina at Chapel Hill Children's Hospital, Chapel Hill (T.C.W., S.P.S.); the Division of Pediatric Critical Care Medicine (E.H.M.) and the Department of Pediatrics (L.S.), Medical University of South Carolina, Charleston; the Division of Pediatric Infectious Diseases, Department of Pediatrics, Children's Mercy Kansas City, Kansas City, MO (J.E.S.); the Departments of Pediatrics and Microbiology, Division of Infectious Diseases, University of Mississippi Medical Center, Jackson (C.V.H.); the Department of Pediatrics, Division of Cardiology, Louisiana State University Health Sciences Center and Children's Hospital of New Orleans, New Orleans (T.T.B.); the Divisions of Pediatric Infectious Diseases and Pediatric Critical Care Medicine, Department of Pediatric and Adolescent Medicine, Mayo Clinic, Rochester (E.R.L.), and the Division of Pediatric Critical Care, University of Minnesota Masonic Children's Hospital, Minneapolis (J.R.H.) - both in Minnesota; the Division of Critical Care Medicine, Department of Anesthesiology and Critical Care, Children's Hospital of Philadelphia, Philadelphia (K.C.); the Ryan White Center for Pediatric Infectious Disease and Global Health, Department of Pediatrics, Indiana University School of Medicine, Indianapolis (S.S.B.); the Division of Pediatric Critical Care Medicine, Children's Hospital of Michigan, Central Michigan University, Detroit (S.M.H.), and the Division of Pediatric Critical Care Medicine, Department of Pediatrics, Mott Children's Hospital and University of Michigan, Ann Arbor (H.R.F.); the Division of Pediatric Critical Care, Department of Pediatrics, Children's Hospital and Medical Center, Omaha, NE (M.L.C.); the Division of Pediatric Critical Care, Department of Pediatrics, Cooperman Barnabas Medical Center, Livingston, NJ (S.J.G.); the Division of Critical Care Medicine, Department of Pediatrics, Northwestern University Feinberg School of Medicine, Ann and Robert H. Lurie Children's Hospital of Chicago, Chicago (B.M. Coates); the Division of Pediatric Critical Care Medicine, Department of Pediatrics, University of Alabama at Birmingham, Birmingham (M.K.); the Division of Pediatric Infectious Diseases, Department of Pediatrics, UHealth Holtz Children's Hospital, Miami (B.M. Chatani); and the Department of Pediatrics and Banner Children's at Diamond Children's Medical Center, University of Arizona, Tucson (K.V.T.).
N Engl J Med. 2022 May 19;386(20):1899-1909. doi: 10.1056/NEJMoa2202826. Epub 2022 Mar 30.
Spread of the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) B.1.1.529 (omicron) variant, which led to increased U.S. hospitalizations for coronavirus disease 2019 (Covid-19), generated concern about immune evasion and the duration of protection from vaccines in children and adolescents.
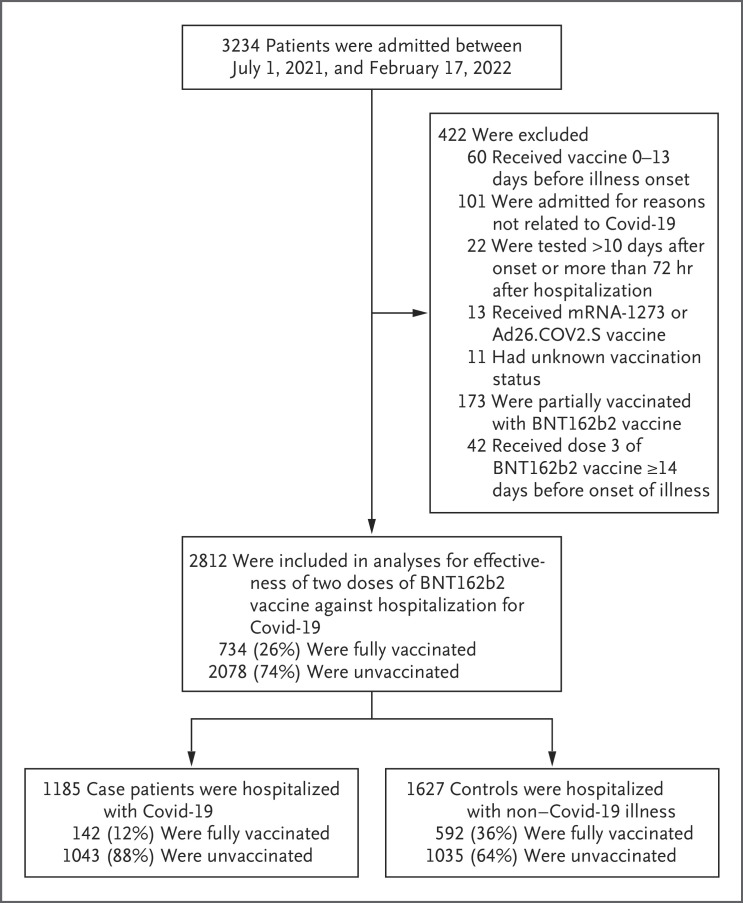
Using a case-control, test-negative design, we assessed vaccine effectiveness against laboratory-confirmed Covid-19 leading to hospitalization and against critical Covid-19 (i.e., leading to receipt of life support or to death). From July 1, 2021, to February 17, 2022, we enrolled case patients with Covid-19 and controls without Covid-19 at 31 hospitals in 23 states. We estimated vaccine effectiveness by comparing the odds of antecedent full vaccination (two doses of BNT162b2 messenger RNA vaccine) at least 14 days before illness among case patients and controls, according to time since vaccination for patients 12 to 18 years of age and in periods coinciding with circulation of B.1.617.2 (delta) (July 1, 2021, to December 18, 2021) and omicron (December 19, 2021, to February 17, 2022) among patients 5 to 11 and 12 to 18 years of age.
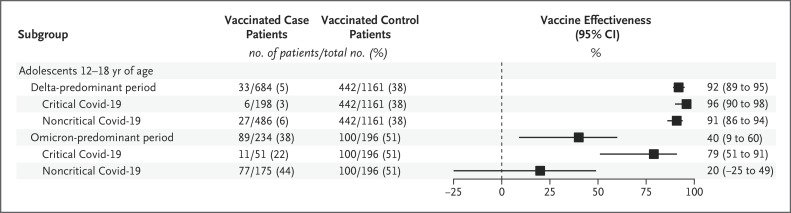
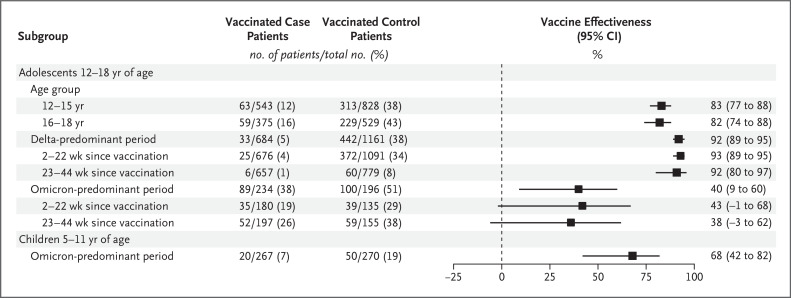
We enrolled 1185 case patients (1043 [88%] of whom were unvaccinated, 291 [25%] of whom received life support, and 14 of whom died) and 1627 controls. During the delta-predominant period, vaccine effectiveness against hospitalization for Covid-19 among adolescents 12 to 18 years of age was 93% (95% confidence interval [CI], 89 to 95) 2 to 22 weeks after vaccination and was 92% (95% CI, 80 to 97) at 23 to 44 weeks. Among adolescents 12 to 18 years of age (median interval since vaccination, 162 days) during the omicron-predominant period, vaccine effectiveness was 40% (95% CI, 9 to 60) against hospitalization for Covid-19, 79% (95% CI, 51 to 91) against critical Covid-19, and 20% (95% CI, -25 to 49) against noncritical Covid-19. During the omicron period, vaccine effectiveness against hospitalization among children 5 to 11 years of age was 68% (95% CI, 42 to 82; median interval since vaccination, 34 days).
BNT162b2 vaccination reduced the risk of omicron-associated hospitalization by two thirds among children 5 to 11 years of age. Although two doses provided lower protection against omicron-associated hospitalization than against delta-associated hospitalization among adolescents 12 to 18 years of age, vaccination prevented critical illness caused by either variant. (Funded by the Centers for Disease Control and Prevention.).
严重急性呼吸系统综合征冠状病毒 2(SARS-CoV-2)B.1.1.529(奥密克戎)变异株的传播导致美国因 2019 年冠状病毒病(COVID-19)而住院的人数增加,这引发了人们对疫苗对儿童和青少年的免疫逃逸和保护持续时间的担忧。
我们使用病例对照、阴性检测设计,评估了疫苗对实验室确诊的 COVID-19 导致住院的有效性,以及对 COVID-19 重症(即需要生命支持或死亡)的有效性。从 2021 年 7 月 1 日至 2022 年 2 月 17 日,我们在 23 个州的 31 家医院招募了 COVID-19 病例患者和未感染 COVID-19 的对照患者。我们根据患者接种疫苗的时间,将 12 至 18 岁患者的疫苗效力与 14 天前至少接受过两剂 BNT162b2 信使 RNA 疫苗的全接种(接种时间在发病前至少 14 天)进行比较,以确定接种疫苗的几率。在 delta 流行期间(2021 年 7 月 1 日至 2021 年 12 月 18 日)和 omicron 流行期间(2021 年 12 月 19 日至 2022 年 2 月 17 日),5 至 11 岁和 12 至 18 岁的患者中,同期存在 B.1.617.2(德尔塔)和 omicron 变异株。
我们共招募了 1185 例病例患者(1043 例[88%]未接种疫苗,291 例[25%]接受生命支持,14 例死亡)和 1627 例对照。在 delta 为主的时期,接种疫苗对 12 至 18 岁青少年因 COVID-19 住院的效力在接种后 2 至 22 周为 93%(95%置信区间[CI],89 至 95),在 23 至 44 周为 92%(95%CI,80 至 97)。在 omicron 为主的时期,12 至 18 岁青少年(接种疫苗后的中位数间隔时间为 162 天),疫苗对 COVID-19 住院的效力为 40%(95%CI,9 至 60),对 COVID-19 重症的效力为 79%(95%CI,51 至 91),对非重症 COVID-19 的效力为 20%(95%CI,-25 至 49)。在 omicron 流行期间,5 至 11 岁儿童接种疫苗对住院的效力为 68%(95%CI,42 至 82;接种疫苗后的中位数间隔时间为 34 天)。
BNT162b2 疫苗将 5 至 11 岁儿童因 omicron 相关住院的风险降低了三分之二。虽然两剂疫苗对 omicron 相关住院的保护作用低于对 delta 相关住院的保护作用,但接种疫苗可以预防任何一种变异引起的重症疾病。(由疾病控制与预防中心资助)。