Gastroenterology and Hepatology Unit, Division of Internal Medicine, Faculty of Medicine, Prince of Songkla University, Hat Yai, 90110, Thailand.
Division of Radiology, Faculty of Medicine, Prince of Songkla University, Hat Yai, 90110, Thailand.
BMC Gastroenterol. 2022 Mar 30;22(1):159. doi: 10.1186/s12876-022-02236-7.
Sarcopenia is associated with disability, mortality, and poorer survival in cirrhotic patients. For the evaluation of muscle volume, computed tomography (CT) is the most accurate tool. Unfortunately, it would be hard to apply a muscle mass measuring CT to daily practice. This research aims to study the utility of handgrip strength (HGS) and bioelectrical impedance analysis (BIA) to detect sarcopenia in cirrhotic patients compared with CT as the reference.
In cirrhotic patients who met inclusions criteria (age 20-70 years, ascites < grade 2 of International Ascites Club grading system, no active malignancy, and no cardiac implanted device), HGS were measured using a Jamar dynamometer. Subsequently, patients with low muscle strength (defined as JSH criteria, < 26 kg in male, < 18 kg in female) were then underwent CT and BIA (Tanita MC780 MA) on the same day to measure muscle volume, the definition of sarcopenia by CT was according to the Japan Society of Hepatology (JSH). We also collected data from patients with normal HGS whose CT results were available in the study period.
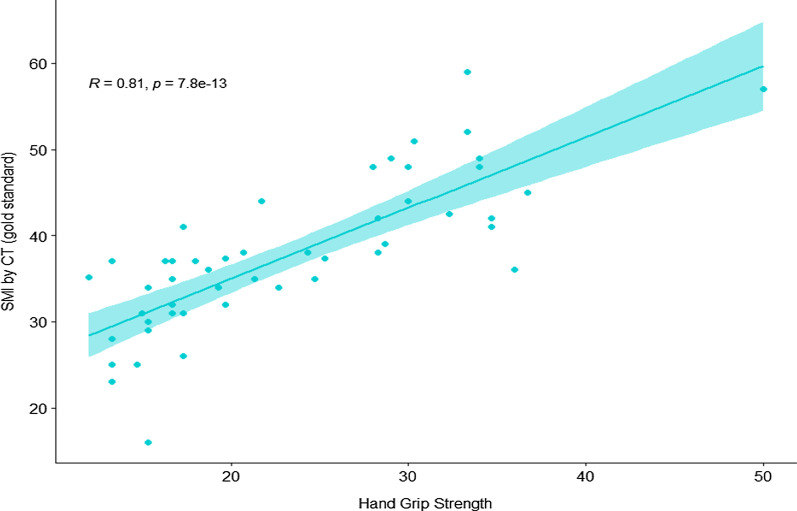
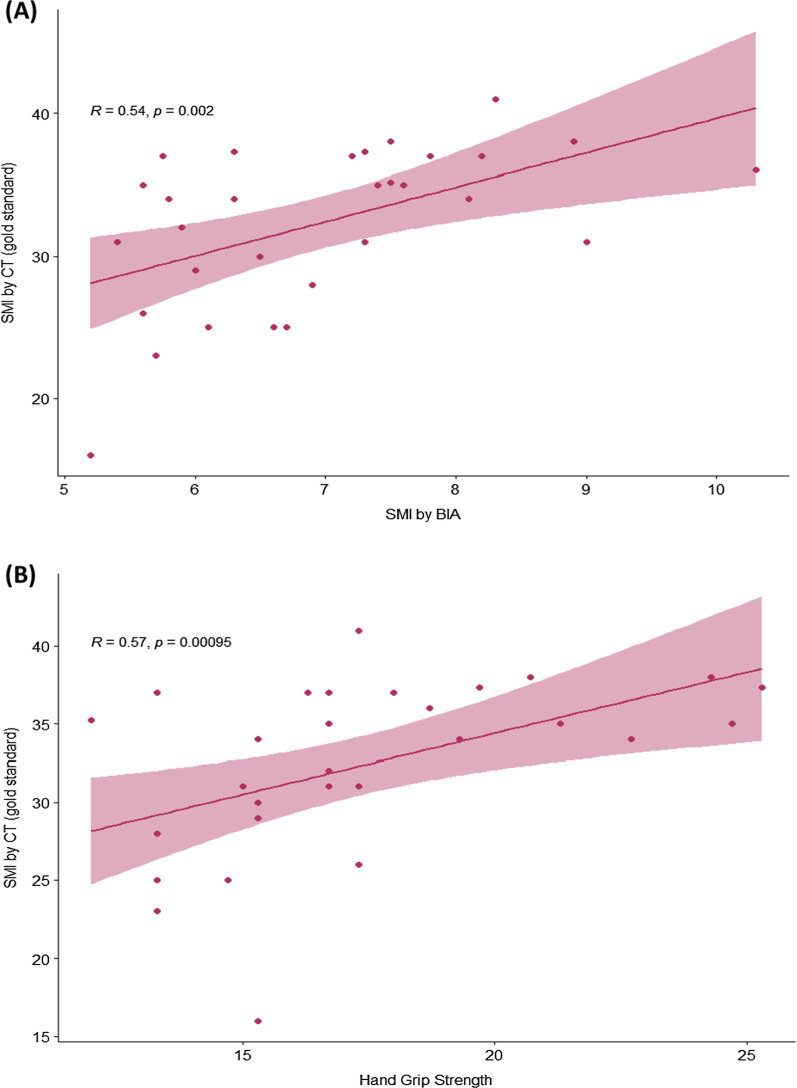
From 146 cirrhotic patients who underwent HGS, 30 patients (20.5%) had diagnosed low HSG. Data from 50 patients whose available CT results included 30 low HGS and 20 patients with normal HSG. The HGS was strongly correlated with skeleton muscle index (SMI) by CT (r = 0.81, p < 0.001) and had an excellent diagnostic performance for detecting sarcopenia by using JSH criteria the sensitivity, specificity, NPV and PPV were 88.2%, 100%, 100%, and 98.7% respectively. In contrast, only 6 of 30 patients (20%) met sarcopenic criteria by BIA. Among sarcopenic patients, the result showed a fair correlation between SMI and BIA (r = 0.54; p < 0.002).
Our study demonstrated an excellent correlation between HGS and SMI by CT in the mixed cirrhotic population from the sarcopenia and non-sarcopenia groups. The HGS using the JSH criteria showed an excellent performance in detecting sarcopenia compared to CT. Nonetheless, for the BIA by using the current cut-offs demonstrated unacceptable rate to detect sarcopenia.
在肝硬化患者中,肌肉减少症与残疾、死亡率和较差的生存相关。对于肌肉量的评估,计算机断层扫描(CT)是最准确的工具。不幸的是,很难将肌肉质量测量 CT 应用于日常实践。本研究旨在研究与 CT 作为参考相比,握力(HGS)和生物电阻抗分析(BIA)检测肝硬化患者肌肉减少症的效用。
在符合纳入标准(年龄 20-70 岁,腹水<国际腹水俱乐部分级系统 2 级,无活动性恶性肿瘤,无心脏植入装置)的肝硬化患者中,使用 Jamar 测力计测量 HGS。随后,肌肉力量较低的患者(根据 JSH 标准定义,男性<26kg,女性<18kg)当天同时进行 CT 和 BIA(Tanita MC780 MA)测量肌肉量,CT 定义的肌肉减少症依据日本肝脏研究学会(JSH)。我们还收集了研究期间 HGS 正常但 CT 结果可用的患者的数据。
在 146 名接受 HGS 检查的肝硬化患者中,有 30 名(20.5%)被诊断为低 HSG。数据来自 50 名患者,其中 30 名 HGS 较低,20 名 HGS 正常。HGS 与 CT 测定的骨骼肌指数(SMI)呈强相关(r=0.81,p<0.001),使用 JSH 标准检测肌肉减少症的诊断性能良好,其敏感性、特异性、NPV 和 PPV 分别为 88.2%、100%、100%和 98.7%。相比之下,仅 30 名患者中的 6 名(20%)符合 BIA 制定的肌肉减少症标准。在肌肉减少症患者中,SMI 和 BIA 之间呈中度相关(r=0.54;p<0.002)。
本研究在肌肉减少症和非肌肉减少症组的混合肝硬化人群中,显示了 HGS 与 CT 测定的 SMI 之间的良好相关性。使用 JSH 标准的 HGS 在检测肌肉减少症方面与 CT 相比表现出优异的性能。然而,对于当前截止值的 BIA,检测肌肉减少症的比例不可接受。