Department of Nursing and Physiotherapy, University of the Balearic Islands, Mallorca, Spain.
Balearic Islands Health Research Institute (IDISBA), Mallorca, Spain.
Scand J Caring Sci. 2022 Dec;36(4):1165-1179. doi: 10.1111/scs.13079. Epub 2022 Mar 31.
A culture of shared leadership is widespread among palliative care teams based on a commitment to valuing and including all people equally. As compassion is a core value for end-of-life care work, compassionate leadership may be the best way to lead in palliative care.
The aims of this study were twofold: (1) to adapt and validate the Compassionate Leadership Self-reported Scale in a sample of palliative care professionals; and (2) to study the relation between compassionate leadership and associated concepts of self-compassion, awareness and self-care.
A cross-sectional survey of 296 Spanish end-of-life care professionals was conducted. Analyses included descriptive statistics, a confirmatory factor analysis (CFA) with four-correlated factors, reliability estimates and a structural model.
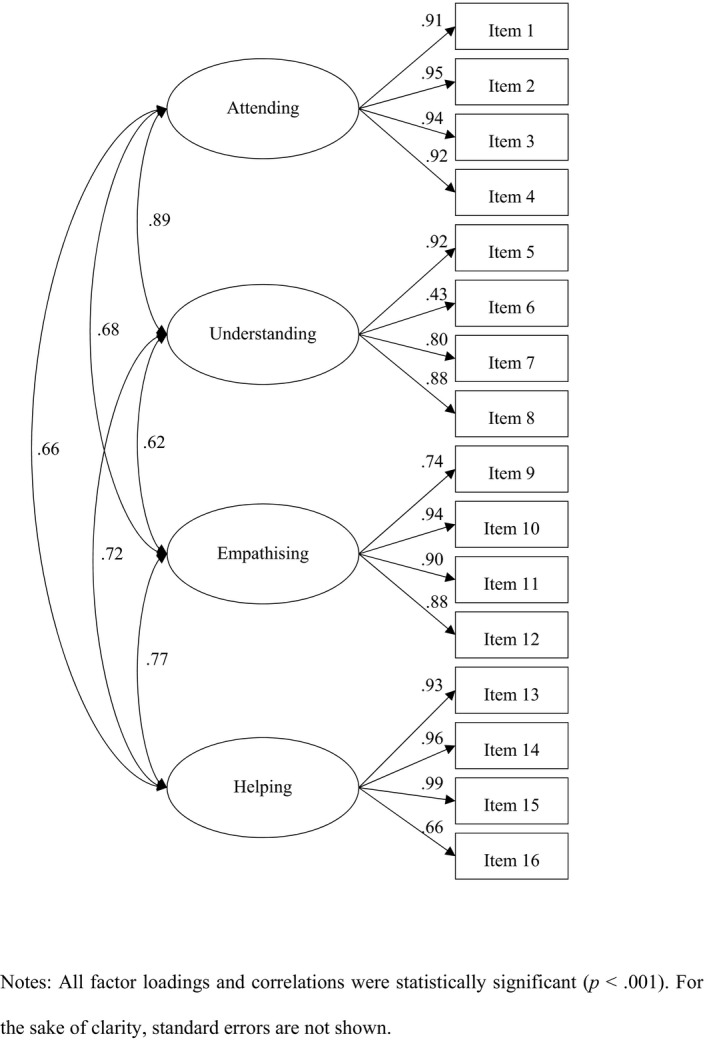
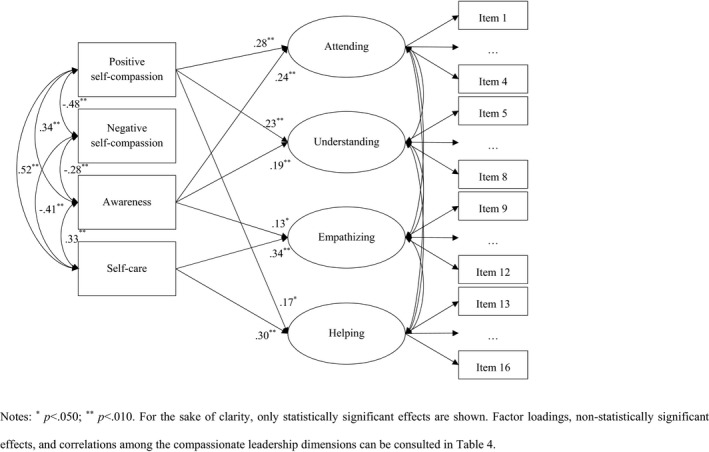
Results suggested there were medium to high levels of compassionate leadership in the sample. The CFA showed an adequate overall fit: χ (98) = 277.595 (p < 0.001); CFI = 0.986; SRMR = 0.047; RMSEA = 0.088 [0.076, 0.100]. Reliability estimates for four subscales of compassionate leadership (attending, understanding, empathising and helping) were also adequate, ranging from 0.72 to 0.96. Finally, the structural model predicting compassionate leadership suggested that the dimensions of attending and understanding were most highly related to positive self-compassion and awareness; empathising, to self-care and awareness; and helping, to positive self-compassion and self-care.
The Compassionate Leadership Scale has adequate psychometric properties when used to assess compassionate leadership in the context of end-of-life care. Our results indicate that self-compassion, awareness and self-care are important correlates of such compassionate leadership.
在以平等重视和包容所有人为宗旨的姑息治疗团队中,共享领导力的文化已普遍存在。由于同情是临终关怀工作的核心价值观,富有同情心的领导可能是姑息治疗的最佳领导方式。
本研究的目的有两个:(1)在姑息治疗专业人员样本中改编和验证《共情领导自我报告量表》;(2)研究共情领导与自我同情、意识和自我关怀等相关概念之间的关系。
对 296 名西班牙临终关怀专业人员进行了横断面调查。分析包括描述性统计、四个相关因素的验证性因素分析(CFA)、信度估计和结构模型。
结果表明,该样本中具有中等至高水平的共情领导能力。CFA 显示出较好的整体拟合度:χ(98)= 277.595(p < 0.001);CFI = 0.986;SRMR = 0.047;RMSEA = 0.088 [0.076,0.100]。共情领导的四个分量表(关注、理解、共情和帮助)的信度估计也足够高,范围在 0.72 到 0.96 之间。最后,预测共情领导的结构模型表明,关注和理解维度与积极的自我同情和意识关系最密切;共情与自我关怀和意识相关;而帮助与积极的自我同情和自我关怀相关。
《共情领导量表》在评估临终关怀背景下的共情领导时具有良好的心理测量学特性。我们的研究结果表明,自我同情、意识和自我关怀是这种共情领导的重要相关因素。