Department of International Health, Bloomberg School of Public Health, Johns Hopkins University, Baltimore, Maryland, USA.
Department of Pediatric Newborn Medicine, Global Advancement of Infants and Mothers (AIM), Brigham and Women's Hospital, Boston, Massachusetts, USA.
J Glob Health. 2022 Mar 26;12:04024. doi: 10.7189/jogh.12.04024. eCollection 2022.
Small for gestational age (SGA) is a public health concern since it is associated with mortality in neonatal and post-neonatal period. Despite the large magnitude of the problem, little is known about the population-attributable risk (PAR) of various risk factors for SGA. This study estimated the relative contribution of risk factors for SGA, as a basis for identifying priority areas for developing and/or implementing interventions to reduce the incidence of SGA births and related mortality and morbidity.
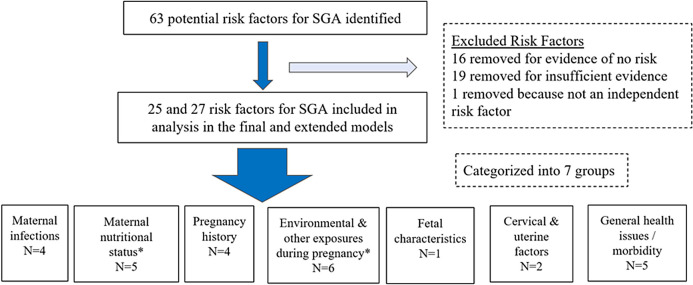
We conducted a literature review on 63 potential risk factors for SGA to quantify the risk relationship and estimate the prevalence of risk factors (RFs). We calculated the population-attributable fraction for each of the identified RF for 81 Countdown countries and calculated regional estimates. Twenty-five RFs were included in the final model while extended model included all the 25 RFs from the final model and two additional RFs.
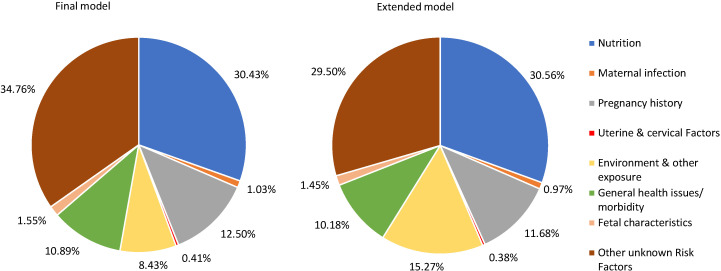
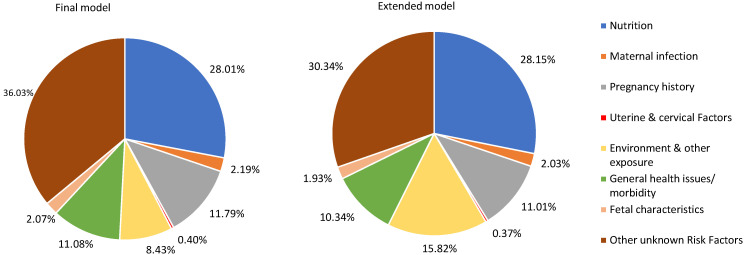
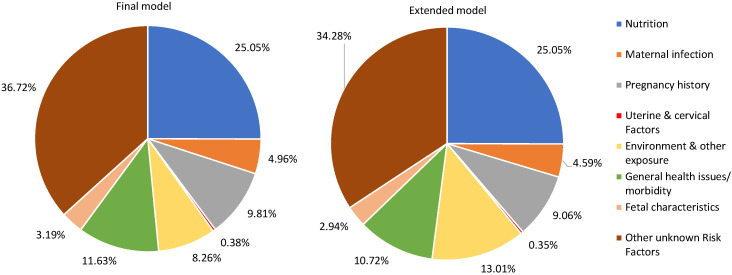
In the final and extended models, the RFs included in each model have a total PAF equal to 63.97% and 69.66%, respectively of SGA across the 81 LMICs. In the extended model, maternal nutritional status has the greatest PAF (28.15%), followed by environmental and other exposures during pregnancy (15.82%), pregnancy history (11.01%), and general health issues or morbidity (10.34%). The RFs included in the final and extended model for Sub-Saharan African (SSA) region have a total PAF of 63.28% and 65.72% of SGA, respectively. In SSA, the top three RF categories in the extended model are nutrition (25.05%), environment and other exposure (13.01%), and general health issues or morbidity (10.72%), while in South-Asia's it was nutrition (30.56%), environment and other exposure (15.27%) and pregnancy history (11.68%).
The various types of RFs that play a role in SGA births highlight the importance of a multifaceted approach to tackle SGA. Depending on the types of RFs, intervention should be strategically targeted at either individual or household and/or community or policy level. There is also a need to research the mechanisms by which some of the RFs might hinder fetal growth.
胎儿生长受限(SGA)是一个公共卫生问题,因为它与新生儿和新生儿后期的死亡率有关。尽管这个问题的规模很大,但对于 SGA 的各种危险因素的人群归因风险(PAR)知之甚少。本研究估计了 SGA 的危险因素的相对贡献,以此为基础确定优先领域,以制定和/或实施干预措施,减少 SGA 出生和相关死亡率和发病率。
我们对 63 种可能导致 SGA 的危险因素进行了文献回顾,以量化风险关系并估计危险因素(RFs)的流行率。我们为 81 个倒计时国家中的每一个确定的 RF 计算了人群归因分数,并计算了区域估计值。在最终模型中,有 25 个 RFs 被纳入,而扩展模型则包括最终模型中的 25 个 RFs 和另外 2 个 RFs。
在最终和扩展模型中,这 81 个中低收入国家的每个模型中的 RFs 的总 PAF 分别为 SGA 的 63.97%和 69.66%。在扩展模型中,孕产妇营养状况的 PAF 最大(28.15%),其次是妊娠期间的环境和其他暴露(15.82%)、妊娠史(11.01%)和一般健康问题或发病率(10.34%)。撒哈拉以南非洲(SSA)地区最终和扩展模型中包含的 RFs 的总 PAF 分别为 SGA 的 63.28%和 65.72%。在 SSA,扩展模型中前三个 RF 类别是营养(25.05%)、环境和其他暴露(13.01%)和一般健康问题或发病率(10.72%),而在南亚,营养(30.56%)、环境和其他暴露(15.27%)和妊娠史(11.68%)是前三个 RF 类别。
导致 SGA 出生的各种 RFs 强调了采取多方面方法解决 SGA 的重要性。根据 RFs 的类型,干预措施应战略性地针对个人或家庭和/或社区或政策层面。还需要研究某些 RFs 可能阻碍胎儿生长的机制。