WorldWide Antimalarial Resistance Network (WWARN), Oxford, UK.
Infectious Diseases Data Observatory (IDDO), Oxford, UK.
BMC Med. 2020 Jun 2;18(1):138. doi: 10.1186/s12916-020-01592-z.
Malaria in pregnancy, including asymptomatic infection, has a detrimental impact on foetal development. Individual patient data (IPD) meta-analysis was conducted to compare the association between antimalarial treatments and adverse pregnancy outcomes, including placental malaria, accompanied with the gestational age at diagnosis of uncomplicated falciparum malaria infection.
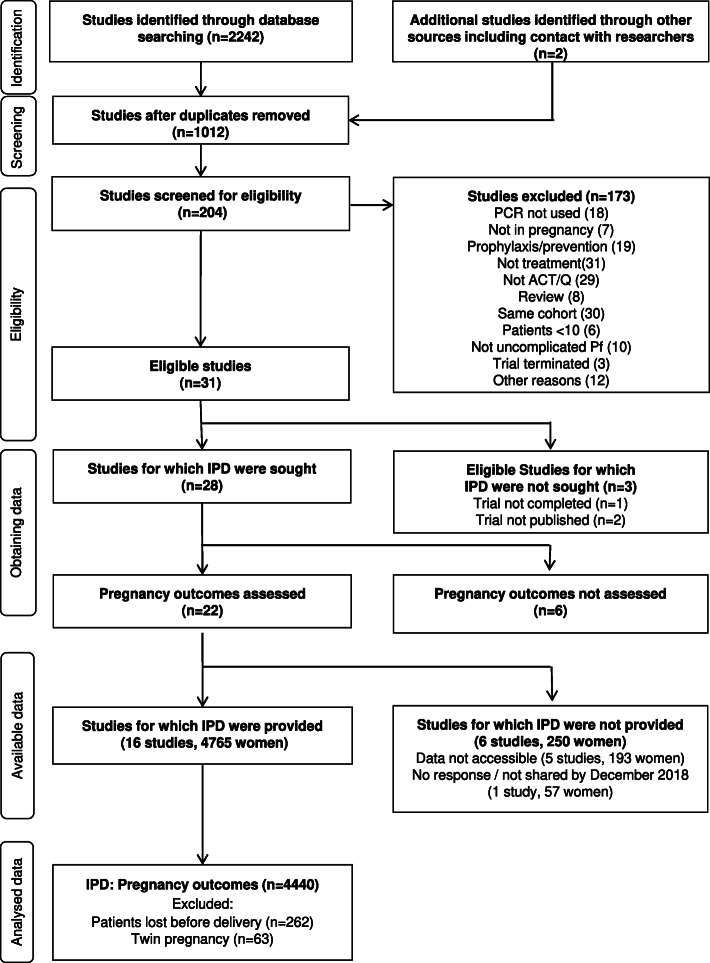
A systematic review and one-stage IPD meta-analysis of studies assessing the efficacy of artemisinin-based and quinine-based treatments for patent microscopic uncomplicated falciparum malaria infection (hereinafter uncomplicated falciparum malaria) in pregnancy was conducted. The risks of stillbirth (pregnancy loss at ≥ 28.0 weeks of gestation), moderate to late preterm birth (PTB, live birth between 32.0 and < 37.0 weeks), small for gestational age (SGA, birthweight of < 10th percentile), and placental malaria (defined as deposition of malaria pigment in the placenta with or without parasites) after different treatments of uncomplicated falciparum malaria were assessed by mixed-effects logistic regression, using artemether-lumefantrine, the most used antimalarial, as the reference standard. Registration PROSPERO: CRD42018104013.
Of the 22 eligible studies (n = 5015), IPD from16 studies were shared, representing 95.0% (n = 4765) of the women enrolled in literature. Malaria treatment in this pooled analysis mostly occurred in the second (68.4%, 3064/4501) or third trimester (31.6%, 1421/4501), with gestational age confirmed by ultrasound in 91.5% (4120/4503). Quinine (n = 184) and five commonly used artemisinin-based combination therapies (ACTs) were included: artemether-lumefantrine (n = 1087), artesunate-amodiaquine (n = 775), artesunate-mefloquine (n = 965), and dihydroartemisinin-piperaquine (n = 837). The overall pooled proportion of stillbirth was 1.1% (84/4361), PTB 10.0% (619/4131), SGA 32.3% (1007/3707), and placental malaria 80.1% (2543/3035), and there were no significant differences of considered outcomes by ACT. Higher parasitaemia before treatment was associated with a higher risk of SGA (adjusted odds ratio [aOR] 1.14 per 10-fold increase, 95% confidence interval [CI] 1.03 to 1.26, p = 0.009) and deposition of malaria pigment in the placenta (aOR 1.67 per 10-fold increase, 95% CI 1.42 to 1.96, p < 0.001).
The risks of stillbirth, PTB, SGA, and placental malaria were not different between the commonly used ACTs. The risk of SGA was high among pregnant women infected with falciparum malaria despite treatment with highly effective drugs. Reduction of malaria-associated adverse birth outcomes requires effective prevention in pregnant women.
妊娠疟疾,包括无症状感染,对胎儿发育有不良影响。进行了个体患者数据(IPD)荟萃分析,以比较不同抗疟治疗方法与不良妊娠结局之间的关联,包括胎盘疟疾,并伴有诊断为无并发症恶性疟原虫感染时的孕龄。
系统评价和一阶段 IPD 荟萃分析评估了基于青蒿素和奎宁的治疗方法在妊娠期间治疗有症状和无症状恶性疟原虫感染(以下简称无并发症恶性疟原虫感染)的疗效。不同治疗方法后死胎(妊娠 28.0 周及以上的妊娠损失)、中度至晚期早产(PTB,活产于 32.0 至 <37.0 周之间)、小于胎龄儿(SGA,出生体重 <第 10 个百分位数)和胎盘疟疾(定义为在胎盘中有或没有寄生虫的疟色素沉积)的风险通过混合效应逻辑回归进行评估,使用青蒿琥酯-咯萘啶作为参考标准。注册 PROSPERO:CRD42018104013。
在 22 项符合条件的研究中(n=5015),16 项研究共享了 IPD,代表了文献中纳入的 95.0%(n=4765)的女性。这组汇总分析中的疟疾治疗主要发生在第二(68.4%,3064/4501)或第三(31.6%,1421/4501)孕期,91.5%(4120/4503)通过超声确认孕龄。纳入了奎宁(n=184)和五种常用的青蒿素类复方疗法(ACT):青蒿琥酯-咯萘啶(n=1087)、青蒿琥酯-阿莫地喹(n=775)、青蒿琥酯-甲氟喹(n=965)和双氢青蒿素-哌喹(n=837)。总的汇总死胎率为 1.1%(84/4361),PTB 为 10.0%(619/4131),SGA 为 32.3%(1007/3707),胎盘疟疾为 80.1%(2543/3035),ACT 之间没有考虑结局的显著差异。治疗前寄生虫血症较高与 SGA 风险增加相关(调整后的优势比[aOR]每增加 10 倍为 1.14,95%置信区间[CI]为 1.03 至 1.26,p=0.009)和胎盘疟色素沉积(aOR 每增加 10 倍为 1.67,95%CI 为 1.42 至 1.96,p<0.001)。
在常用的 ACT 之间,死胎、PTB、SGA 和胎盘疟疾的风险没有差异。尽管使用了高效药物,感染恶性疟原虫的孕妇仍存在 SGA 风险高的问题。减少与疟疾相关的不良出生结局需要对孕妇进行有效的预防。