Lee Anne Cc, Workneh Firehiwot, Kang Yunhee, Yibeltal Kalkidan, Fasil Nebiyou, Tsegaye Sitota, Baye Estifanos, Kidane Workagegnehu Tarekegn, Berhane Yoseph Yemane, Derebe Mulatu Melese, Van Dyk Fred, Eglovitch Michelle, Olson Ingrid, Mengistie Mandefro M, Shiferie Fisseha, Shifraw Tigest, Lu Chunling, North Krysten, Chan Grace J, Isanaka Sheila, Molina Rose L, Tadesse Amare Worku, Wylie Blair J, Christian Parul, Mullany Luke C, Worku Alemayehu, Berhane Yemane
Department of Pediatrics, Brown University, Providence, Rhode Island, USA
Department of Pediatrics, Brigham and Women's Hospital, Boston, Massachusetts, USA.
BMJ Glob Health. 2025 Jun 18;10(6):e016264. doi: 10.1136/bmjgh-2024-016264.
We aimed to determine the impact of antenatal interventions to optimise maternal nutrition and infection management on birth outcomes in Ethiopia.
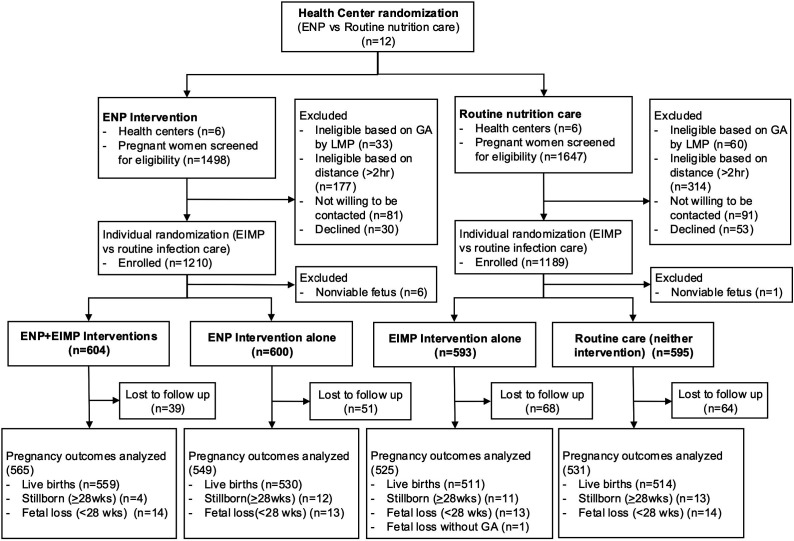
We conducted a pragmatic, open-label, 2×2 factorial randomised clinical effectiveness study among pregnant women enrolled <24 weeks gestation in 12 rural health centres in Amhara, Ethiopia. Eligible health centres were randomised to deliver an enhanced nutrition package (ENP) (iron-folic acid, iodised salt and targeted micronutrient fortified balanced energy protein (BEP) supplementation for undernourished women) or routine nutrition care (iron-folic acid only). Individual women were randomised to receive an enhanced infection management package (EIMP) (genitourinary tract infection screening-treatment and enhanced deworming) or routine infection care (syndromic management). The primary outcomes were birth weight and length; secondary outcomes were gestational age, preterm delivery, small-for-gestational-age, low birth weight, stillbirth, newborn weight-for-age and length-for-age z-scores, newborn head circumference, and maternal anemia. Analysis was intention to treat.
From August 2020 to December 2021, 2392 women were randomised (604 ENP+EIMP, 600 ENP alone, 593 EIMP alone and 595 neither package) and followed until June 2022, with 2170 pregnancy outcomes analysed (565 ENP+EIMP, 549 ENP, 525 EIMP, 531 neither). In the ENP arm, 427 (36%) women were eligible for BEP and consumed on average 74 days. The prevalence of genitourinary tract infection was low (4.9%), while parasitic stool infections were common (31%). There was no difference in birth weight (ENP vs not-ENP: adjusted mean difference -4 g (-83 to 75); EIMP vs not-EIMP: 18 g (-35 to 70); ENP+EIMP vs neither: 14 g (-81 to 109)) or birth length (ENP: -0.3 cm (-1.1 to 0.5); EIMP: 0.2 cm (-0.1 to 0.5); ENP+EIMP: -0.1 cm (-1.2 to 1.1)) between study arms. In the ENP+EIMP group, the stillbirth rate was lower compared with the arm receiving neither package (7.1/1000 vs 24.7/1000 births; adjusted relative risk: 0.29 (0.09 to 0.94)). The packages did not significantly affect other secondary outcomes.
In this pragmatic study implemented within the Ethiopian health system, enhanced nutrition and infection packages did not affect birth weight or length. While stillbirth rates were lower in the group receiving both packages, these findings need to be supported by additional studies.
ISRCTN15116516.
我们旨在确定产前干预措施对优化孕产妇营养和感染管理,从而对埃塞俄比亚出生结局的影响。
我们在埃塞俄比亚阿姆哈拉地区12个农村卫生中心对妊娠小于24周的孕妇开展了一项实用、开放标签的2×2析因随机临床有效性研究。符合条件的卫生中心被随机分配提供强化营养套餐(ENP)(铁-叶酸、碘盐以及针对营养不良妇女的靶向微量营养素强化平衡能量蛋白(BEP)补充剂)或常规营养护理(仅铁-叶酸)。个体妇女被随机分配接受强化感染管理套餐(EIMP)(泌尿生殖道感染筛查-治疗以及强化驱虫)或常规感染护理(症状管理)。主要结局为出生体重和身长;次要结局为孕周、早产、小于胎龄儿、低出生体重、死产、新生儿年龄别体重和年龄别身长Z评分、新生儿头围以及孕产妇贫血。分析采用意向性治疗。
2020年8月至2021年12月,2392名妇女被随机分组(604名接受ENP+EIMP,600名仅接受ENP,593名仅接受EIMP,595名两者均未接受)并随访至2022年6月,共分析了2170例妊娠结局(565例ENP+EIMP,549例ENP,525例EIMP,531例两者均未接受)。在ENP组中,427名(36%)妇女符合BEP条件且平均服用74天。泌尿生殖道感染患病率较低(4.9%),而寄生虫粪便感染很常见(31%)。各研究组之间在出生体重(ENP组与非ENP组:调整后平均差异-4克(-83至75);EIMP组与非EIMP组:18克(-35至70);ENP+EIMP组与两者均未接受组:14克(-81至109))或出生身长(ENP组:-0.3厘米(-1.1至0.5);EIMP组:0.2厘米(-0.1至0.5);ENP+EIMP组:-0.1厘米(-1.2至1.1))方面无差异。在ENP+EIMP组中,与两者均未接受组相比,死产率较低(7.1/1000例分娩与24.7/1000例分娩;调整后相对风险:0.29(0.09至0.94))。这些套餐对其他次要结局无显著影响。
在埃塞俄比亚卫生系统内开展的这项实用研究中,强化营养和感染套餐未影响出生体重或身长。虽然接受两种套餐的组死产率较低,但这些结果需要更多研究予以支持。
ISRCTN15116516