Institute for Healthcare Policy and Innovation, University of Michigan, Ann Arbor.
Department of Emergency Medicine, University of Michigan, Ann Arbor.
JAMA Netw Open. 2022 Mar 1;5(3):e225484. doi: 10.1001/jamanetworkopen.2022.5484.
During the COVID-19 pandemic, many primary care practices adopted telehealth in place of in-person care to preserve access to care for patients with acute and chronic conditions. The extent to which this change was associated with their rates of acute care visits (ie, emergency department visits and hospitalizations) for these conditions is unknown.
To examine whether a primary care practice's level of telehealth use is associated with a change in their rate of acute care visits for ambulatory care-sensitive conditions (ACSC visits).
DESIGN, SETTING, AND PARTICIPANTS: This retrospective cohort analysis used a difference-in-differences study design to analyze insurance claims data from 4038 Michigan primary care practices from January 1, 2019, to September 30, 2020.
Low, medium, or high tertile of practice-level telehealth use based on the rate of telehealth visits from March 1 to August 31, 2020, compared with prepandemic visit volumes.
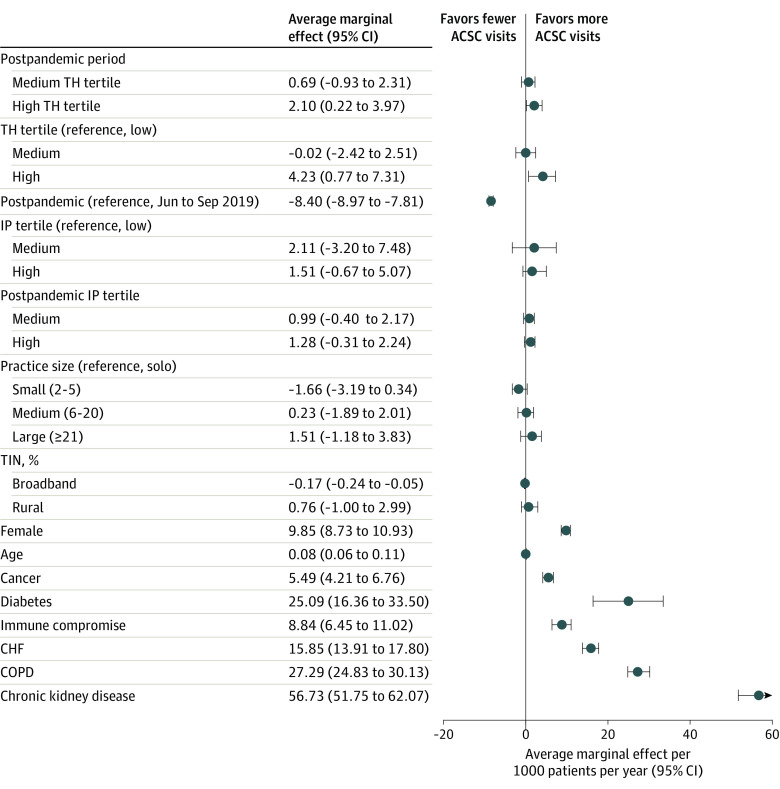
Risk-adjusted ACSC visit rates before (June to September 2019) and after (June to September 2020) the start of the COVID-19 pandemic, reported as an annualized average marginal effect. The study examined overall, acute, and chronic ACSC visits separately and controlled for practice size, in-person visit volume, zip code-level attributes, and patient characteristics.
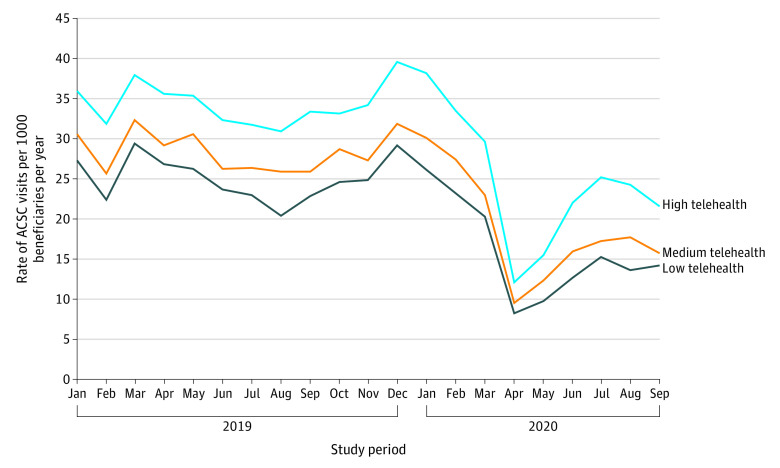
A total of nearly 1.5 million beneficiaries (53% female; mean [SD] age, 40 [22] years) were attributed to 4038 primary care practices. Compared with 2019 visit volumes, median telehealth use was 0.4% for the low telehealth tertile, 14.7% for the medium telehealth tertile, and 39.0% for the high telehealth tertile. The number of ACSC visits decreased in all tertiles, with adjusted rates changing from 24.3 to 14.9 per 1000 patients per year (low), 23.9 to 15.3 per 1000 patients per year (medium), and 27.5 to 20.2 per 1000 patients per year (high). In difference-in-differences analysis, high telehealth use was associated with a higher ACSC visit rate (2.10 more visits per 1000 patients per year; 95% CI, 0.22-3.97) compared with low telehealth practices; practices in the middle tertile did not differ significantly from the low tertile. No difference was found in ACSC visits across tertiles when acute and chronic ACSC visits were examined separately.
In this cohort study that used a difference-in-differences analysis, the association between practice-level telehealth use and ACSC visits was mixed. High telehealth use was associated with a slightly higher overall ACSC visit rate than low telehealth practices. The association of telehealth with downstream care use should be closely monitored going forward.
在 COVID-19 大流行期间,许多初级保健实践采用远程医疗代替面对面护理,以维持患有急性和慢性疾病的患者获得护理的机会。这种变化与他们这些疾病的急性护理就诊率(即急诊就诊和住院)之间的关联程度尚不清楚。
检查初级保健实践的远程医疗使用水平是否与他们的急性护理就诊率(即 ACSC 就诊)的变化相关。
设计、地点和参与者:这是一项回顾性队列分析,采用差异中的差异研究设计,分析了 2019 年 1 月 1 日至 2020 年 9 月 30 日来自密歇根州 4038 家初级保健实践的保险索赔数据。
与大流行前就诊量相比,基于 2020 年 3 月 1 日至 8 月 31 日的实践水平远程医疗就诊率,分为低、中、高三分位组。
大流行开始前后(2019 年 6 月至 9 月)的 ACSC 就诊率,以每年平均边际效应的形式报告。该研究分别对整体、急性和慢性 ACSC 就诊进行了研究,并控制了实践规模、面对面就诊量、邮政编码级别属性和患者特征。
共有近 150 万受益人(53%为女性;平均[SD]年龄为 40[22]岁)归因于 4038 家初级保健实践。与 2019 年就诊量相比,低远程医疗三分位数的中位远程医疗使用率为 0.4%,中远程医疗三分位数为 14.7%,高远程医疗三分位数为 39.0%。所有三分位数的 ACSC 就诊次数均减少,调整后的就诊率从每年每 1000 名患者 24.3 次降至 14.9 次(低)、每年每 1000 名患者 23.9 次降至 15.3 次(中)和每年每 1000 名患者 27.5 次降至 20.2 次(高)。在差异中的差异分析中,与低远程医疗实践相比,高远程医疗使用率与 ACSC 就诊率较高相关(每年每 1000 名患者多 2.10 次就诊;95%CI,0.22-3.97);中间三分位数的实践与低三分位数无显著差异。在分别检查急性和慢性 ACSC 就诊时,在 ACSC 就诊的三分位数之间没有发现差异。
在这项使用差异中的差异分析的队列研究中,实践层面远程医疗使用与 ACSC 就诊之间的关联是混合的。高远程医疗使用率与低远程医疗实践相比,总体 ACSC 就诊率略高。应密切监测远程医疗与下游护理使用之间的关联。