Chereshnev Valeriy A, Pichugova Svetlana V, Beikin Yakov B, Chereshneva Margarita V, Iukhta Angelina I, Stroev Yuri I, Churilov Leonid P
Institute of Immunology and Physiology, Ural Branch of the Russian Academy of Sciences, 620049 Yekaterinburg, Russia.
State Autonomous Healthcare Institution of the Sverdlovsk Region "Clinical and Diagnostic Center" (GAUZ SO "CDC" Clinical Diagnostic Center), 620144 Yekaterinburg, Russia.
Pathophysiology. 2021 Oct 15;28(4):471-488. doi: 10.3390/pathophysiology28040030.
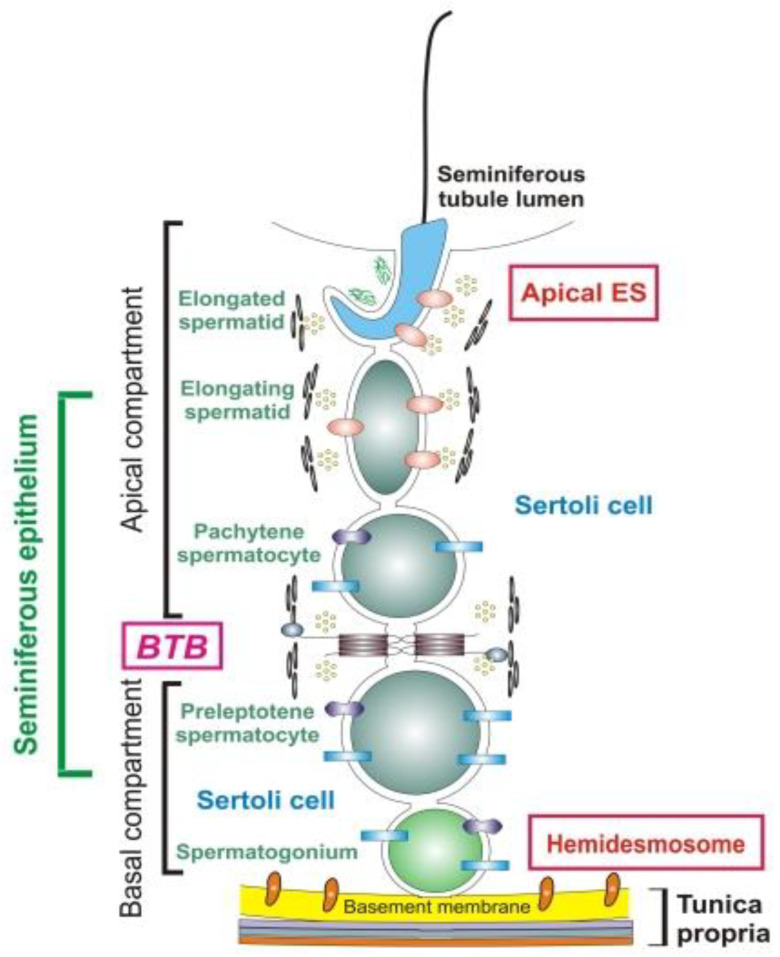
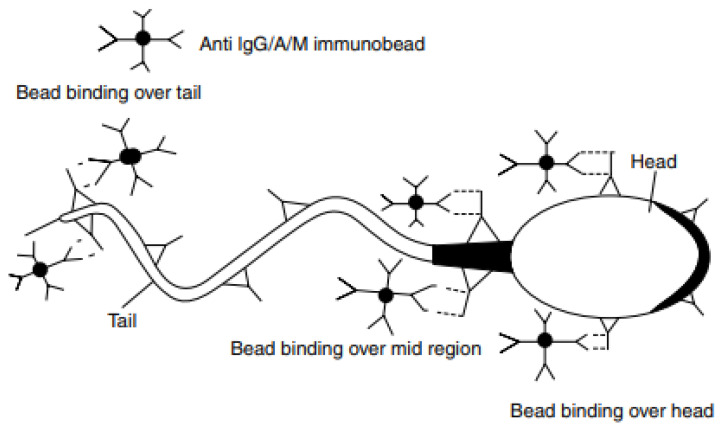
According to global data, there is a male reproductive potential decrease. Pathogenesis of male infertility is often associated with autoimmunity towards sperm antigens essential for fertilization. Antisperm autoantibodies (ASAs) have immobilizing and cytotoxic properties, impairing spermatogenesis, causing sperm agglutination, altering spermatozoa motility and acrosomal reaction, and thus preventing ovum fertilization. Infertility diagnosis requires a mandatory check for the ASAs. The concept of the blood-testis barrier is currently re-formulated, with an emphasis on informational paracrine and juxtacrine effects, rather than simple anatomical separation. The etiology of male infertility includes both autoimmune and non-autoimmune diseases but equally develops through autoimmune links of pathogenesis. Varicocele commonly leads to infertility due to testicular ischemic damage, venous stasis, local hyperthermia, and hypoandrogenism. However, varicocelectomy can alter the blood-testis barrier, facilitating ASAs production as well. There are contradictory data on the role of ASAs in the pathogenesis of varicocele-related infertility. Infection and inflammation both promote ASAs production due to "danger concept" mechanisms and because of antigen mimicry. Systemic pro-autoimmune influences like hyperprolactinemia, hypoandrogenism, and hypothyroidism also facilitate ASAs production. The diagnostic value of various ASAs has not yet been clearly attributed, and their cut-levels have not been determined in sera nor in ejaculate. The assessment of the autoimmunity role in the pathogenesis of male infertility is ambiguous, so the purpose of this review is to show the effects of ASAs on the pathogenesis of male infertility.
根据全球数据,男性生殖潜能有所下降。男性不育的发病机制通常与针对受精所必需的精子抗原的自身免疫有关。抗精子自身抗体(ASAs)具有制动和细胞毒性特性,会损害精子发生,导致精子凝集,改变精子活力和顶体反应,从而阻止卵子受精。不育诊断需要强制性检查ASAs。血睾屏障的概念目前正在重新阐述,重点在于信息旁分泌和邻分泌效应,而非简单的解剖学分离。男性不育的病因包括自身免疫性和非自身免疫性疾病,但同样通过发病机制的自身免疫联系发展而来。精索静脉曲张通常由于睾丸缺血性损伤、静脉淤滞、局部高温和雄激素缺乏而导致不育。然而,精索静脉结扎术也会改变血睾屏障,从而促进ASAs的产生。关于ASAs在精索静脉曲张相关性不育发病机制中的作用,存在相互矛盾的数据。感染和炎症由于“危险概念”机制以及抗原模拟作用,都会促进ASAs的产生。系统性的促自身免疫影响,如高泌乳素血症、雄激素缺乏和甲状腺功能减退,也会促进ASAs的产生。各种ASAs的诊断价值尚未明确确定,其在血清和精液中的临界值也未确定。自身免疫在男性不育发病机制中的作用评估尚不明确,因此本综述的目的是展示ASAs对男性不育发病机制的影响。