Division of Cardiovascular Medicine (Drs Shea and Pack and Mr Schilling), Institute for Healthcare Delivery and Population Science (Drs Headley and Pack), and Department of Medicine (Dr Pack), University of Massachusetts Medical School-Baystate, Springfield; Springfield College Department of Exercise Science and Athletic Training, Springfield, Massachusetts (Drs Shea, Headley, and Mullin); Mayo Clinic Arizona, Scottsdale (Dr Shea); and Division of Cardiovascular Medicine, Henry Ford Hospital, Detroit, Michigan (Dr Brawner).
J Cardiopulm Rehabil Prev. 2022 Sep 1;42(5):352-358. doi: 10.1097/HCR.0000000000000682. Epub 2022 Mar 31.
Although ratings of perceived exertion (RPE) are widely used to guide exercise intensity in cardiac rehabilitation (CR), it is unclear whether target heart rate ranges (THRRs) can be implemented in CR programs that predominantly use RPE and what impact this has on changes in exercise capacity.
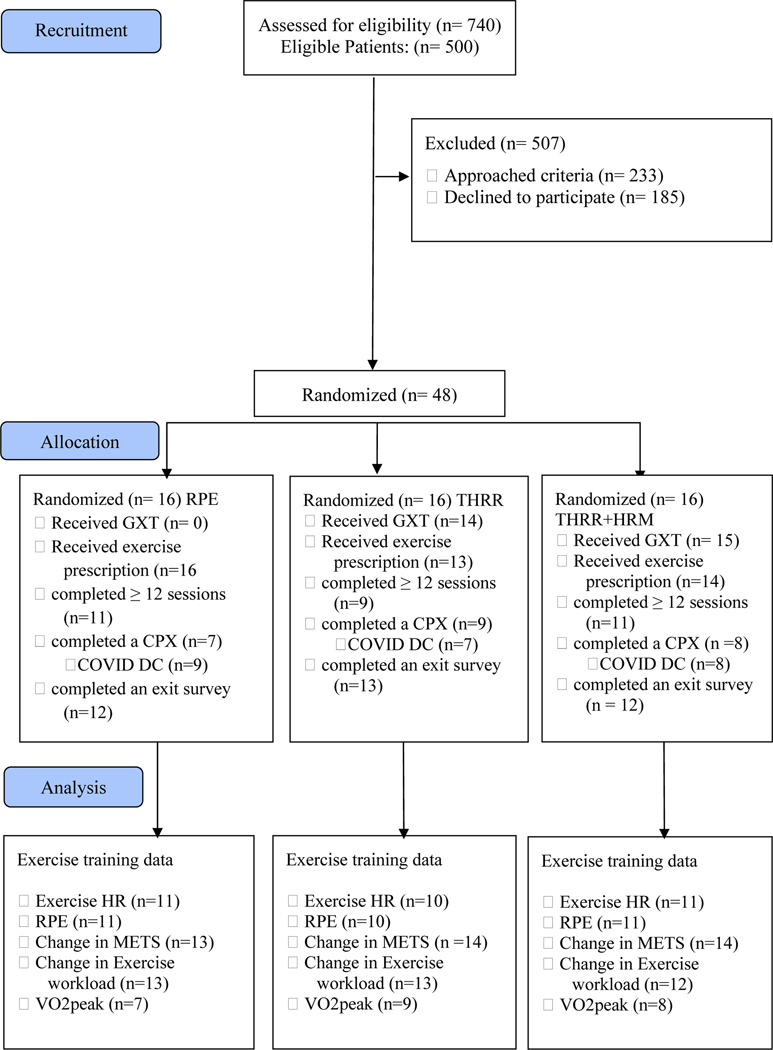
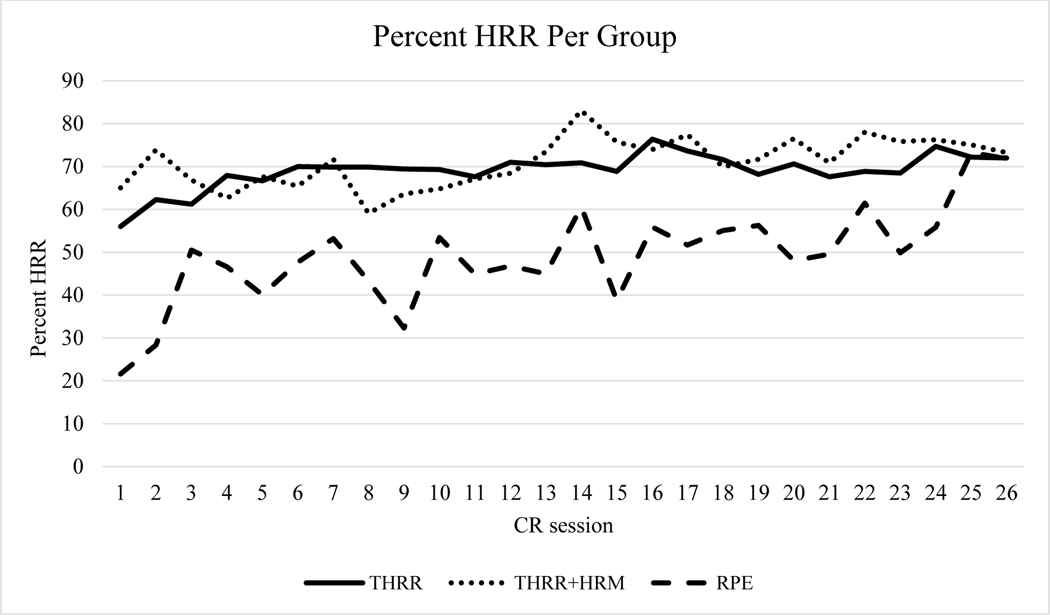
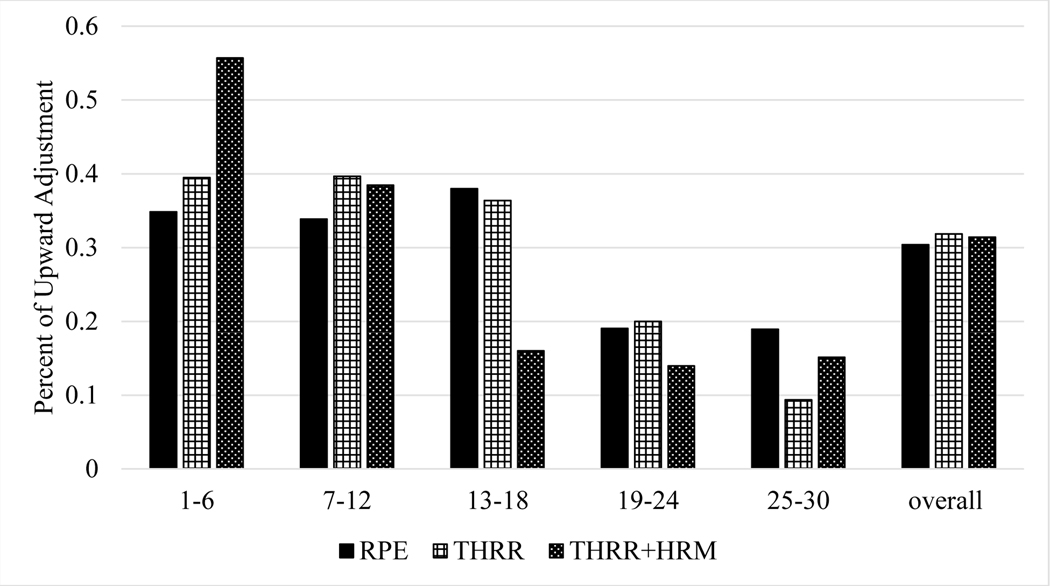
We conducted a three-group pilot randomized control trial (#NCT03925493) comparing RPE of 3-4 on the 10-point modified Borg scale, 60-80% of heart rate reserve (HRR) with heart rate (HR) monitored by telemetry, or 60-80% of HRR with a personal HR monitor (HRM) for high-fidelity adherence to THRR. Primary outcomes were protocol fidelity and feasibility. Secondary outcomes included exercise HR, RPE, and changes in functional exercise capacity.
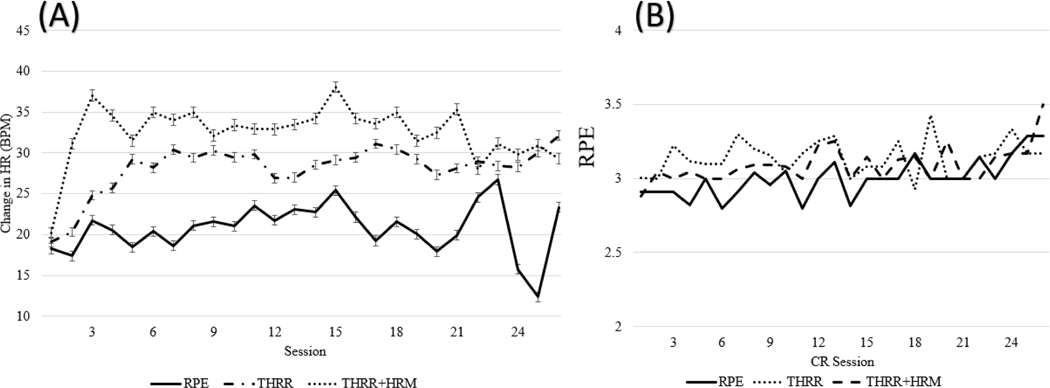
Of 48 participants randomized, four patients dropped out, 20 stopped prematurely (COVID-19 pandemic), and 24 completed the protocol. Adherence to THRR was high regardless of HRM, and patients attended a median (IQR) of 33 (23, 36) sessions with no difference between groups. After randomization, HR increased by 1 ± 6, 6 ± 5, and 10 ± 9 bpm ( P = .02); RPE (average score 3.0 ± 0.05) was unchanged, and functional exercise capacity increased by 1.0 ± 1.0, 1.9 ± 1.5, 2.0 ± 1.3 workload METs (effect size between groups, ηp2 = 0.11, P = .20) for the RPE, THRR, and THRR + HRM groups, respectively.
We successfully implemented THRR in an all-RPE CR program without needing an HRM. Patients randomized to THRR had higher exercise HR but similar RPE ratings. The THRR may be preferable to RPE in CR populations for cardiorespiratory fitness gains, but this needs confirmation in an adequately powered trial.
尽管感知用力程度(RPE)评分被广泛用于指导心脏康复(CR)中的运动强度,但尚不清楚在主要使用 RPE 的 CR 计划中是否可以实施目标心率范围(THRR),以及这对运动能力的变化有何影响。
我们进行了一项三组前瞻性随机对照试验(#NCT03925493),比较了 10 点改良 Borg 量表的 3-4 级 RPE、通过遥测监测的心率储备(HRR)的 60-80%、或个人 HR 监测仪(HRM)的 60-80% HRR,以实现对 THRR 的高保真依从性。主要结局是方案的忠实度和可行性。次要结局包括运动时的心率、RPE 和功能运动能力的变化。
在随机分配的 48 名患者中,有 4 名患者退出,20 名患者提前退出(COVID-19 大流行),24 名患者完成了方案。无论使用 HRM 如何,对 THRR 的依从性都很高,并且患者参加了中位数(IQR)为 33(23,36)次的治疗,各组之间无差异。随机分组后,HR 分别增加了 1±6、6±5 和 10±9 bpm(P=0.02);RPE(平均评分为 3.0±0.05)保持不变,功能运动能力分别增加了 1.0±1.0、1.9±1.5 和 2.0±1.3 瓦尔特(workload METs)(组间效应大小,ηp2=0.11,P=0.20),分别为 RPE、THRR 和 THRR+HRM 组。
我们成功地在完全使用 RPE 的 CR 计划中实施了 THRR,而无需 HRM。随机分配到 THRR 的患者运动时心率更高,但 RPE 评分相似。对于心肺适能的提高,THRR 可能优于 CR 人群中的 RPE,但这需要在一项充分有力的试验中得到证实。