Norwegian Research Center for Women's Health, Oslo University Hospital, Oslo, Norway.
Institute of Clinical Medicine, University of Oslo, Oslo, Norway.
Acta Obstet Gynecol Scand. 2022 Jul;101(7):819-826. doi: 10.1111/aogs.14358. Epub 2022 Apr 7.
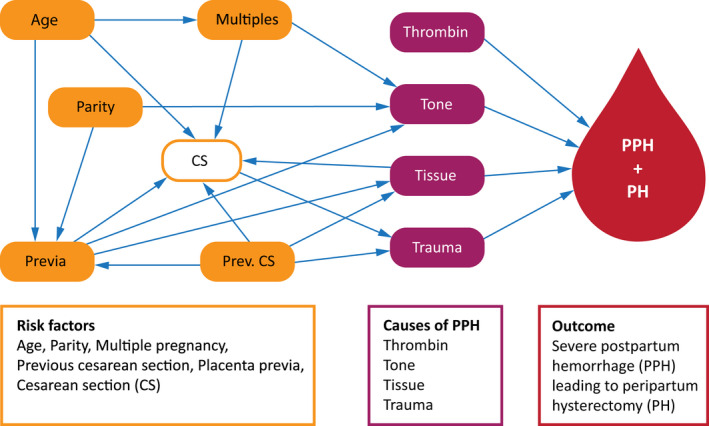
A peripartum hysterectomy is typically performed as a lifesaving procedure in obstetrics to manage severe postpartum hemorrhage. Severe hemorrhages that lead to peripartum hysterectomies are mainly caused by uterine atony and placenta accreta spectrum disorders. In this study, we aimed to estimate the incidence, risk factors, causes and management of severe postpartum hemorrhage resulting in peripartum hysterectomies, and to describe the complications of the hysterectomies.
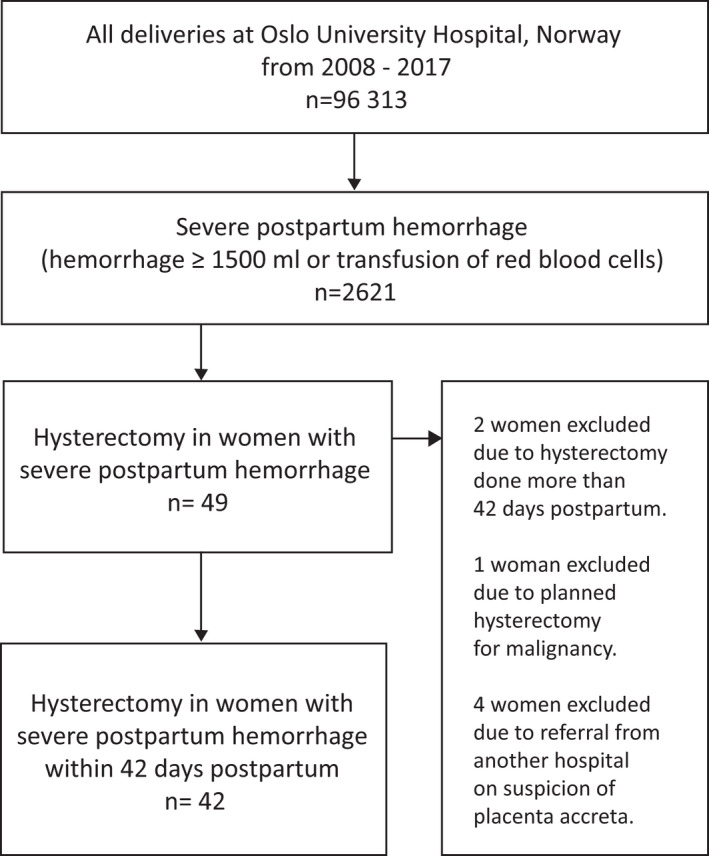
Eligible women had given birth at gestational week 23+0 or later and had a postpartum hemorrhage ≥1500 mL or a blood transfusion, due to postpartum hemorrhage, at Oslo University Hospital, Norway, between 2008 and 2017. Among the eligible women, this study included those who underwent a hysterectomy within the first 42 days after delivery. The Norwegian Medical Birth Registry provided the reference group. We used Poisson regression to estimate adjusted incidence rate ratios with 95% confidence intervals to identify clinical factors associated with peripartum hysterectomy.
The incidence of hysterectomies with severe postpartum hemorrhage was 0.44/1000 deliveries (42/96313). Among the women with severe postpartum hemorrhage, 1.6% ended up with a hysterectomy (42/2621). Maternal age ≥40, previous cesarean section, multiple pregnancy and placenta previa were associated with a significantly higher risk of hysterectomy. Placenta accreta spectrum disorders were the most frequent cause of hemorrhage that resulted in a hysterectomy (52%, 22/42) and contributed to most of the complications following the hysterectomy (11/15 women with complications).
The rate of peripartum hysterectomies at Oslo University Hospital was low, but was higher than previously reported from Norway. Risk factors included high maternal age, previous cesarean section, multiple pregnancy and placenta previa, well known risk factors for placenta accreta spectrum disorders and severe postpartum hemorrhage. Placenta accreta spectrum disorders were the largest contributor to hysterectomies and complications.
围产期子宫切除术通常是产科中用于治疗严重产后出血的救命手术。导致围产期子宫切除术的严重出血主要由子宫收缩乏力和胎盘植入谱系疾病引起。在这项研究中,我们旨在估计导致围产期子宫切除术的严重产后出血的发生率、危险因素、原因和处理方法,并描述子宫切除术的并发症。
符合条件的女性在挪威奥斯陆大学医院分娩,孕周 23+0 或以上,产后出血≥1500ml 或因产后出血需要输血,在 2008 年至 2017 年期间,符合条件的女性中,本研究包括那些在分娩后 42 天内接受子宫切除术的女性。挪威医学出生登记处提供了参考组。我们使用泊松回归估计调整后的发病率比和 95%置信区间,以确定与围产期子宫切除术相关的临床因素。
严重产后出血行子宫切除术的发生率为 0.44/1000 分娩(42/96313)。在严重产后出血的女性中,1.6%(42/2621)最终行子宫切除术。产妇年龄≥40 岁、既往剖宫产、多胎妊娠和前置胎盘与子宫切除术的风险显著增加相关。胎盘植入谱系疾病是导致子宫切除术的出血最常见原因(52%,22/42),并导致子宫切除术后的大多数并发症(15 名有并发症的女性中有 11 名)。
奥斯陆大学医院的围产期子宫切除术发生率较低,但高于挪威以前的报告。危险因素包括高龄产妇、既往剖宫产、多胎妊娠和前置胎盘,这些都是胎盘植入谱系疾病和严重产后出血的已知危险因素。胎盘植入谱系疾病是导致子宫切除术和并发症的最大原因。