Wańha Wojciech, Tomaniak Mariusz, Wańczura Piotr, Bil Jacek, Januszek Rafał, Wolny Rafał, Opolski Maksymilian P, Kuźma Łukasz, Janas Adam, Figatowski Tomasz, Gąsior Paweł, Milewski Marek, Roleder-Dylewska Magda, Lewicki Łukasz, Kulczycki Jan, Włodarczak Adrian, Tomasiewicz Brunon, Iwańczyk Sylwia, Sacha Jerzy, Koltowski Łukasz, Dziarmaga Miłosz, Jaguszewski Miłosz, Kralisz Paweł, Olajossy Bartosz, Sobieszek Grzegorz, Dyrbuś Krzysztof, Łebek Mariusz, Smolka Grzegorz, Reczuch Krzysztof, Gil Robert J, Dobrzycki Sławomir, Kwiatkowski Piotr, Rogala Marcin, Gąsior Mariusz, Ochała Andrzej, Kochman Janusz, Witkowski Adam, Lesiak Maciej, D'Ascenzo Fabrizio, Bartuś Stanisław, Wojakowski Wojciech
Department of Cardiology and Structural Heart Diseases, Medical University of Silesia, 40-055 Katowice, Poland.
1st Department of Cardiology, Medical University of Warsaw, 02-091 Warszawa, Poland.
J Clin Med. 2022 Mar 23;11(7):1779. doi: 10.3390/jcm11071779.
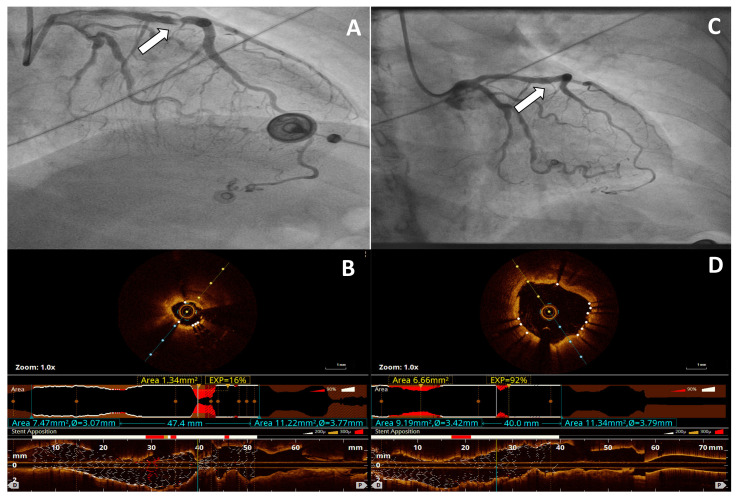
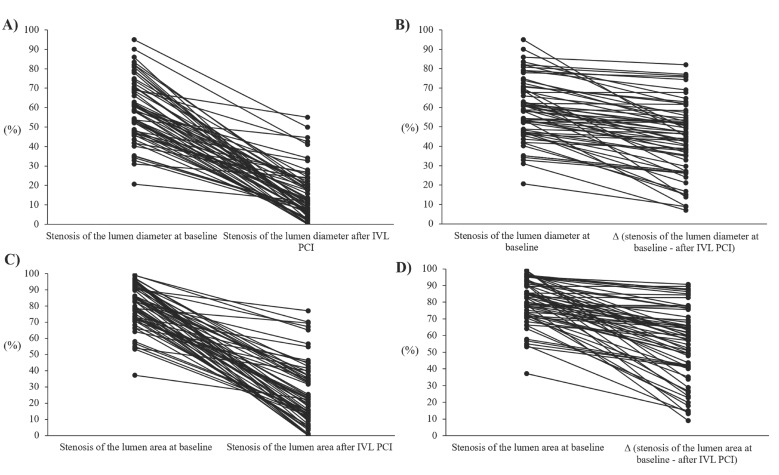
Background: Whereas the efficacy and safety of intravascular lithotripsy (IVL) have been confirmed in de novo calcified coronary lesions, little is known about its utility in treating stent underexpansion. This study aimed to investigate the impact of IVL in treating stent underexpansion. Methods and Results: Consecutive patients with stent underexpansion treated with IVL entered the multicenter IVL-Dragon Registry. The procedural success (primary efficacy endpoint) was defined as a relative stent expansion >80%. Thirty days device-oriented composite endpoint (DOCE) (defined as a composite of cardiac death, target lesion revascularization, or target vessel myocardial infarction) was the secondary endpoint. A total of 62 patients were enrolled. The primary efficacy endpoint was achieved in 72.6% of patients. Both stent underexpansion 58.5% (47.5−69.7) vs. 11.4% (5.8−20.7), p < 0.001, and the stenotic area 82.6% (72.4−90.8) vs. 21.5% (11.1−37.2), p < 0.001, measured by quantitative coronary angiography improved significantly after IVL. Intravascular imaging confirmed increased stent expansion following IVL from 37.5% (16.0−66.0) to 86.0% (69.2−90.7), p < 0.001, by optical coherence tomography and from 57.0% (31.5−77.2) to 89.0% (85.0−92.0), p = 0.002, by intravascular ultrasound. Secondary endpoint occurred in one (1.6%) patient caused by cardiac death. There was no target lesion revascularization or target vessel myocardial infarction during the 30-day follow-up. Conclusions: In this real-life, largest-to-date analysis of IVL use to manage underexpanded stent, IVL proved to be an effective and safe method for facilitating stent expansion and increasing luminal gain.
血管内碎石术(IVL)在初发钙化冠状动脉病变中的疗效和安全性已得到证实,但其在治疗支架扩张不全方面的应用知之甚少。本研究旨在探讨IVL对治疗支架扩张不全的影响。方法与结果:连续接受IVL治疗的支架扩张不全患者进入多中心IVL-Dragon注册研究。手术成功(主要疗效终点)定义为支架相对扩张>80%。30天器械导向复合终点(DOCE)(定义为心源性死亡、靶病变血运重建或靶血管心肌梗死的复合终点)为次要终点。共纳入62例患者。72.6%的患者达到主要疗效终点。通过定量冠状动脉造影测量,支架扩张不全情况从58.5%(47.5−69.7)降至11.4%(5.8−20.7),p<0.001,狭窄面积从82.6%(72.4−90.8)降至21.5%(11.1−37.2),p<0.001,IVL治疗后均有显著改善。血管内成像证实,通过光学相干断层扫描,IVL后支架扩张从37.5%(16.0−66.0)增加到86.0%(69.2−90.7),p<0.001,通过血管内超声从57.0%(31.5−77.2)增加到89.0%(85.0−92.0),p = 0.002。次要终点发生在1例(1.6%)因心源性死亡的患者中。30天随访期间无靶病变血运重建或靶血管心肌梗死发生。结论:在这项关于IVL用于处理扩张不全支架的现实生活中规模最大的分析中,IVL被证明是促进支架扩张和增加管腔增益的有效且安全的方法。