Huang Zheng-Yang, Liu Yong, Huang Hao-Fan, Huang Shu-Hua, Wang Jing-Xin, Tian Jin-Fei, Zeng Wen-Xian, Lv Rong-Gui, Jiang Song, Gao Jun-Ling, Gao Yi, Yu Xia-Xia
School of Biomedical Engineering, Health Science Center, Shenzhen University, Shenzhen 518037, Guangdong Province, China.
Intensive Care Unit, Shenzhen Hospital, Southern Medical University, Shenzhen 518101, Guangdong Province, China.
World J Clin Cases. 2022 Mar 26;10(9):2751-2763. doi: 10.12998/wjcc.v10.i9.2751.
The exact definition of Acute kidney injury (AKI) for patients with traumatic brain injury (TBI) is unknown.
To compare the power of the "Risk, Injury, Failure, Loss of kidney function, and End-stage kidney disease" (RIFLE), Acute Kidney Injury Network (AKIN), Creatinine kinetics (CK), and Kidney Disease Improving Global Outcomes (KDIGO) to determine AKI incidence/stage and their association with the in-hospital mortality rate of patients with TBI.
This retrospective study collected the data of patients admitted to the intensive care unit for neurotrauma from 2001 to 2012, and 1648 patients were included. The subjects in this study were assessed for the presence and stage of AKI using RIFLE, AKIN, CK, and KDIGO. In addition, the propensity score matching method was used.
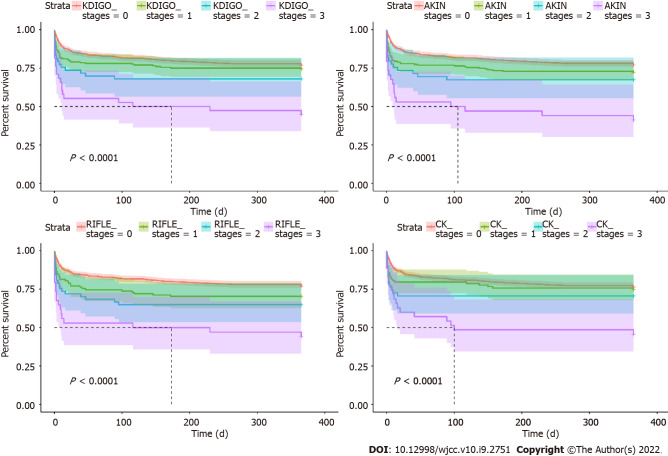
Among the 1648 patients, 291 (17.7%) had AKI, according to KDIGO. The highest incidence of AKI was found by KDIGO (17.7%), followed by AKIN (17.1%), RIFLE (12.7%), and CK (11.5%) ( = 0.97). Concordance between KDIGO and RIFLE/AKIN/CK was 99.3%/99.1%/99.3% for stage 0, 36.0%/91.5%/44.5% for stage 1, 35.9%/90.6%/11.3% for stage 2, and 47.4%/89.5%/36.8% for stage 3. The in-hospital mortality rates increased with the AKI stage in all four definitions. The severity of AKI by all definitions and stages was not associated with in-hospital mortality in the multivariable analyses (all > 0.05).
Differences are seen in AKI diagnosis and in-hospital mortality among the four AKI definitions or stages. This study revealed that KDIGO is the best method to define AKI in patients with TBI.
创伤性脑损伤(TBI)患者急性肾损伤(AKI)的确切定义尚不清楚。
比较“风险、损伤、衰竭、肾功能丧失和终末期肾病”(RIFLE)、急性肾损伤网络(AKIN)、肌酐动力学(CK)和改善全球肾脏病预后组织(KDIGO)在确定AKI发生率/分期方面的效能及其与TBI患者院内死亡率的关联。
这项回顾性研究收集了2001年至2012年入住重症监护病房的神经创伤患者的数据,共纳入1648例患者。本研究中的受试者使用RIFLE、AKIN、CK和KDIGO评估AKI的存在情况和分期。此外,采用了倾向评分匹配法。
根据KDIGO标准,在1648例患者中,291例(17.7%)发生AKI。KDIGO发现的AKI发生率最高(17.7%),其次是AKIN(17.1%)、RIFLE(12.7%)和CK(11.5%)(P = 0.97)。KDIGO与RIFLE/AKIN/CK在0期的一致性为99.3%/99.1%/99.3%,1期为36.0%/91.5%/44.5%,2期为35.9%/90.6%/11.3%,3期为47.4%/89.5%/36.8%。在所有四种定义中,院内死亡率均随AKI分期增加。在多变量分析中,所有定义和分期的AKI严重程度均与院内死亡率无关(所有P>0.05)。
四种AKI定义或分期在AKI诊断和院内死亡率方面存在差异。本研究表明,KDIGO是定义TBI患者AKI的最佳方法。