Luo Xuying, Jiang Li, Du Bin, Wen Ying, Wang Meiping, Xi Xiuming
Crit Care. 2014 Jul 8;18(4):R144. doi: 10.1186/cc13977.
Recently, the Kidney Disease: Improving Global Outcomes (KDIGO) proposed a new definition and classification of acute kidney injury (AKI) on the basis of the RIFLE (Risk, Injury, Failure, Loss of kidney function, and End-stage renal failure) and AKIN (Acute Kidney Injury Network) criteria, but comparisons of the three criteria in critically ill patients are rare.
We prospectively analyzed a clinical database of 3,107 adult patients who were consecutively admitted to one of 30 intensive care units of 28 tertiary hospitals in Beijing from 1 March to 31 August 2012. AKI was defined by the RIFLE, AKIN, and KDIGO criteria. Receiver operating curves were used to compare the predictive ability for mortality, and logistic regression analysis was used for the calculation of odds ratios and 95% confidence intervals.
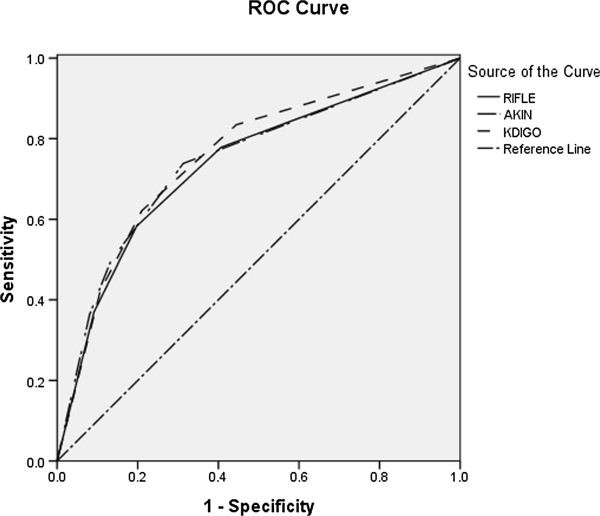
The rates of incidence of AKI using the RIFLE, AKIN, and KDIGO criteria were 46.9%, 38.4%, and 51%, respectively. KDIGO identified more patients than did RIFLE (51% versus 46.9%, P = 0.001) and AKIN (51% versus 38.4%, P <0.001). Compared with patients without AKI, in-hospital mortality was significantly higher for those diagnosed as AKI by using the RIFLE (27.8% versus 7%, P <0.001), AKIN (32.2% versus 7.1%, P <0.001), and KDIGO (27.4% versus 5.6%, P <0.001) criteria, respectively. There was no difference in AKI-related mortality between RIFLE and KDIGO (27.8% versus 27.4%, P = 0.815), but there was significant difference between AKIN and KDIGO (32.2% versus 27.4%, P = 0.006). The areas under the receiver operator characteristic curve for in-hospital mortality were 0.738 (P <0.001) for RIFLE, 0.746 (P <0.001) for AKIN, and 0.757 (P <0.001) for KDIGO. KDIGO was more predictive than RIFLE for in-hospital mortality (P <0.001), but there was no difference between KDIGO and AKIN (P = 0.12).
A higher incidence of AKI was diagnosed according to KDIGO criteria. Patients diagnosed as AKI had a significantly higher in-hospital mortality than non-AKI patients, no matter which criteria were used. Compared with the RIFLE criteria, KDIGO was more predictive for in-hospital mortality, but there was no significant difference between AKIN and KDIGO.
最近,改善全球肾脏病预后组织(KDIGO)基于RIFLE(风险、损伤、衰竭、肾功能丧失和终末期肾衰竭)和急性肾损伤网络(AKIN)标准提出了急性肾损伤(AKI)的新定义和分类,但在危重病患者中对这三种标准进行比较的研究较少。
我们前瞻性分析了2012年3月1日至8月31日期间连续入住北京28家三级医院30个重症监护病房之一的3107例成年患者的临床数据库。AKI分别根据RIFLE、AKIN和KDIGO标准进行定义。采用受试者工作特征曲线比较对死亡率的预测能力,并采用逻辑回归分析计算比值比和95%置信区间。
按照RIFLE、AKIN和KDIGO标准,AKI的发生率分别为46.9%、38.4%和51%。KDIGO识别出的患者比RIFLE(51%对46.9%,P = 0.001)和AKIN(51%对38.4%,P <0.001)更多。与未发生AKI的患者相比,按照RIFLE(27.8%对7%,P <0.001)、AKIN(32.2%对7.1%,P <0.001)和KDIGO(27.4%对5.6%,P <0.001)标准诊断为AKI的患者院内死亡率显著更高。RIFLE和KDIGO之间在AKI相关死亡率方面无差异(27.8%对27.4%,P = 0.815),但AKIN和KDIGO之间存在显著差异(32.2%对27.4%,P = 0.006)。RIFLE、AKIN和KDIGO预测院内死亡率的受试者工作特征曲线下面积分别为0.738(P <0.001)、0.746(P <0.001)和0.757(P <0.001)。KDIGO对院内死亡率的预测性高于RIFLE(P <0.001),但KDIGO和AKIN之间无差异(P = 0.12)。
根据KDIGO标准诊断出的AKI发生率更高。无论采用哪种标准,诊断为AKI的患者院内死亡率均显著高于非AKI患者。与RIFLE标准相比,KDIGO对院内死亡率的预测性更强,但AKIN和KDIGO之间无显著差异。