Division of Cardiology, Department of Medicine, Johns Hopkins Hospital, Carnegie 568D, 600 N. Wolfe St. Baltimore, MD, USA.
Cardiovascular Genetics Center, Montreal Heart Institute, Université de Montréal, 5000 Bélanger St, Montréal, Canada.
Eur Heart J. 2022 Aug 21;43(32):e1-e9. doi: 10.1093/eurheartj/ehac180.
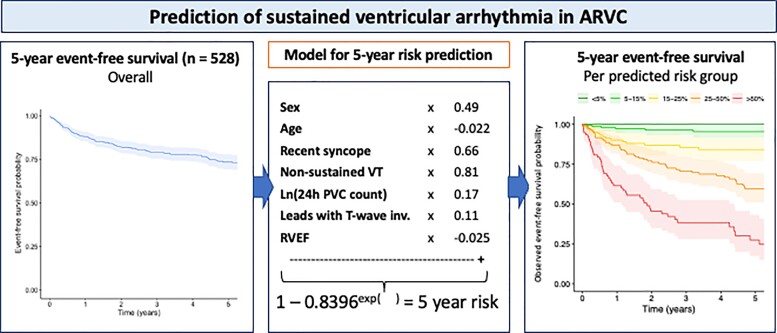
Arrhythmogenic right ventricular dysplasia/cardiomyopathy (ARVC) is characterized by ventricular arrhythmias (VAs) and sudden cardiac death (SCD). We aimed to develop a model for individualized prediction of incident VA/SCD in ARVC patients.
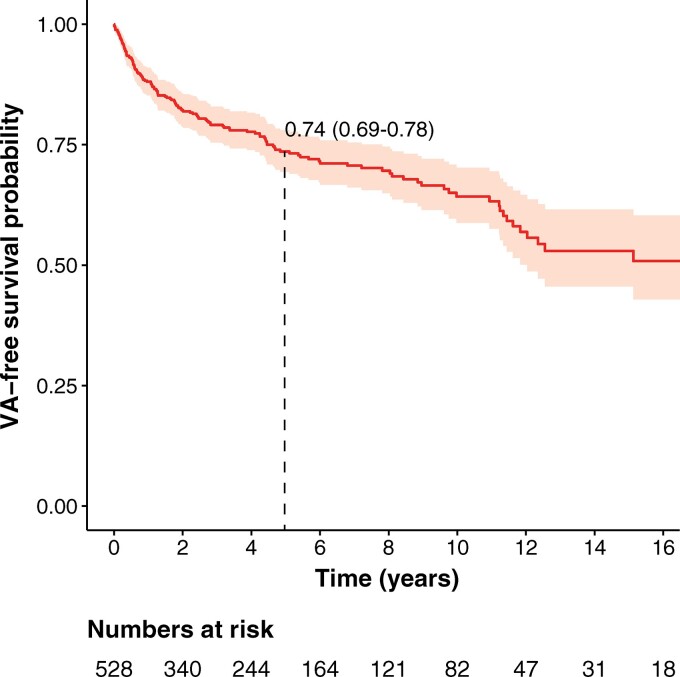
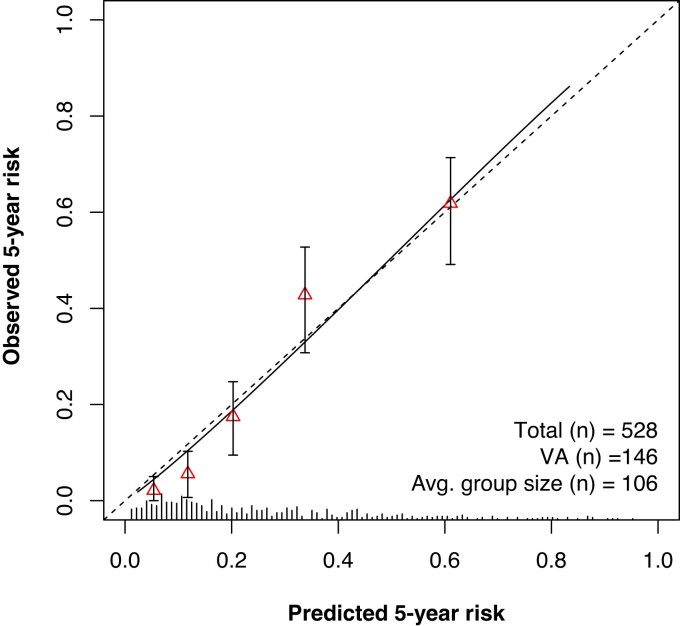
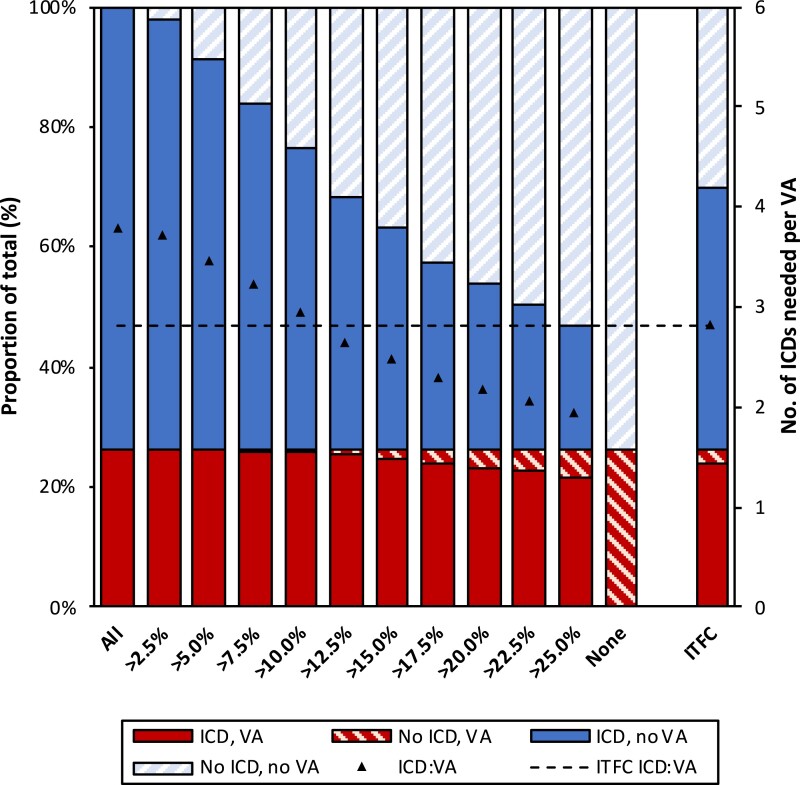
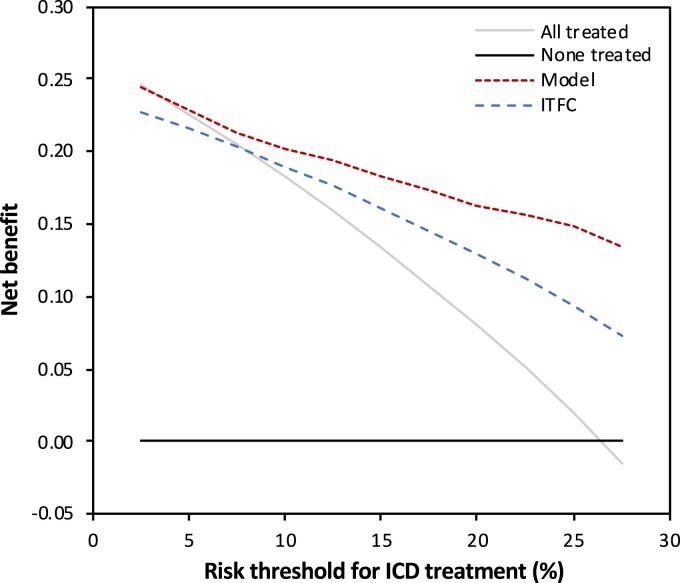
Five hundred and twenty-eight patients with a definite diagnosis and no history of sustained VAs/SCD at baseline, aged 38.2 ± 15.5 years, 44.7% male, were enrolled from five registries in North America and Europe. Over 4.83 (interquartile range 2.44-9.33) years of follow-up, 146 (27.7%) experienced sustained VA, defined as SCD, aborted SCD, sustained ventricular tachycardia, or appropriate implantable cardioverter-defibrillator (ICD) therapy. A prediction model estimating annual VA risk was developed using Cox regression with internal validation. Eight potential predictors were pre-specified: age, sex, cardiac syncope in the prior 6 months, non-sustained ventricular tachycardia, number of premature ventricular complexes in 24 h, number of leads with T-wave inversion, and right and left ventricular ejection fractions (LVEFs). All except LVEF were retained in the final model. The model accurately distinguished patients with and without events, with an optimism-corrected C-index of 0.77 [95% confidence interval (CI) 0.73-0.81] and minimal over-optimism [calibration slope of 0.93 (95% CI 0.92-0.95)]. By decision curve analysis, the clinical benefit of the model was superior to a current consensus-based ICD placement algorithm with a 20.3% reduction of ICD placements with the same proportion of protected patients (P < 0.001).
Using the largest cohort of patients with ARVC and no prior VA, a prediction model using readily available clinical parameters was devised to estimate VA risk and guide decisions regarding primary prevention ICDs (www.arvcrisk.com).
致心律失常性右室心肌病(ARVC)的特征是室性心律失常(VA)和心脏性猝死(SCD)。我们旨在建立一种预测 ARVC 患者发生 VA/SCD 的个体化模型。
本研究纳入了来自北美和欧洲五个登记处的 528 名明确诊断且基线时无持续性 VA/SCD 病史的患者,年龄为 38.2±15.5 岁,其中 44.7%为男性。在 4.83 年(四分位距 2.44-9.33)的随访期间,146 名患者(27.7%)经历了持续性 VA,定义为 SCD、SCD 中止、持续性室性心动过速或适当的植入式心脏复律除颤器(ICD)治疗。采用 Cox 回归和内部验证建立了预测 VA 年风险的模型。预先指定了 8 个潜在预测因子:年龄、性别、过去 6 个月的心脏性晕厥、非持续性室性心动过速、24 小时内的室性期前收缩数、T 波倒置导联数和右心室和左心室射血分数(LVEF)。除 LVEF 外,其余因子均保留在最终模型中。该模型能准确区分有和无事件的患者,经校正后的 optimism-corrected C 指数为 0.77(95%CI 0.73-0.81),且最小化了过度乐观的情况[校准斜率为 0.93(95%CI 0.92-0.95)]。通过决策曲线分析,该模型的临床获益优于当前基于共识的 ICD 放置算法,在相同比例的受保护患者中,可减少 20.3%的 ICD 放置(P<0.001)。
本研究使用了最大的 ARVC 患者队列,且患者无先前的 VA,开发了一种使用易于获得的临床参数预测 VA 风险的模型,以指导关于原发性预防 ICD 的决策(www.arvcrisk.com)。