Jianyang Hospital of Traditional Chinese Medicine, Jianyang, 641400, China.
Hospital of Chengdu University of Traditional Chinese Medicine, Chengdu, 610072, China.
BMC Endocr Disord. 2022 Apr 20;22(1):106. doi: 10.1186/s12902-022-00997-6.
The accumulation of advanced glycation end products (AGEs) occurring in skin tissues can be measured by AGE Reader. Here, we assessed the correlation between AGEs values and the development of type 2 diabetic peripheral neuropathy (DPN).
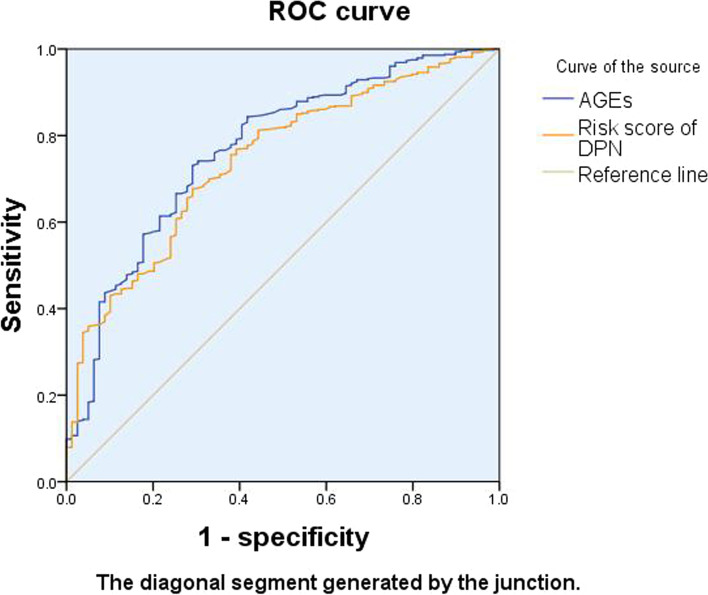
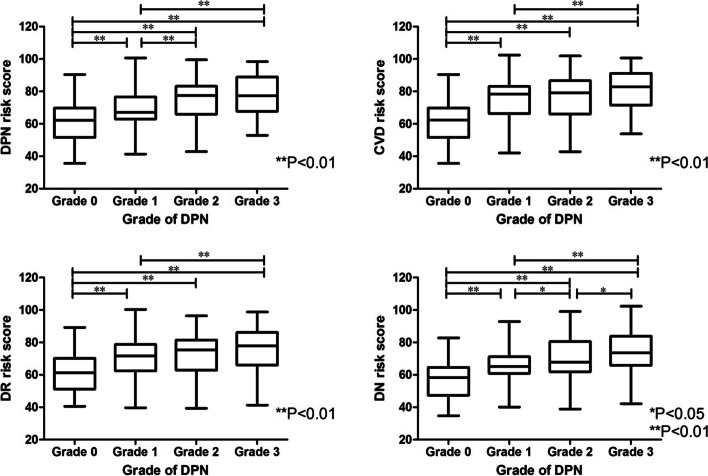
The basic clinical information of 560 patients with T2DM was collected through an electronic system. AGEs and diabetic complication risk score was measured by AGE Reader, a non-invasive optical signal detector. All of the participants were classified into 4 groups based on Dyck criteria: grade 0 (non-DPN group), grade 1 (early stage group), grade 2 (middle stage group) and grade 3 (advanced group). Pearson correlation analysis and Spearman correlation analysis were used to evaluate the correlation between AGEs and other indexes. The sensitivity and specificity of glycosylated products were evaluated by ROC curve.
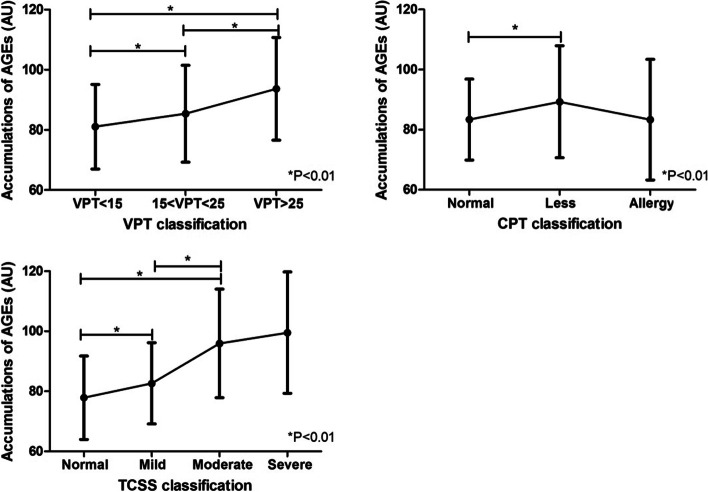
With the increase of DPN severity, the accumulative AGEs showed an increasing trend. Significant differences (P = 0.000) of AGEs were found among grades 0, 1, 2, and 3 of DPN, and significant differences (P = 0.000) of AGEs were found between grades 1 and 3. There were significant differences in DPN risk score between grades 0, 1, 2, and 3, between grades 1, 2, and 3, and between grades 2 and 3 (P < 0.01 or P < 0.05). AGEs were positively correlated with age, blood uric acid, disease course, systolic blood pressure, the risk scores of the four major complications of diabetes, renal function indicators (serum creatinine, Cystatin C, homocysteine, the ratio of urinary albumin and creatinine, urinary microalbumin, α-microglobulin, urinary transferrin, urinary immunoglobulin), inflammatory indicators (white blood cell count, neutrophil count, neutrophil-to-lymphocyte ratio, C-reactive protein), and TCSS score. However, it was negatively correlated with BMI,fasting insulin, insulin 1-3 h postprandial, lymphocyte count, HOMA insulin resistance index and estimated glomerular filtration rate. The area under the AGEs cumulant and neuropathy risk score curve was 0.769 and 0.743, respectively. The confidence intervals were (71.2-82.6%) and (68.8-79.9%), respectively. The maximum Youden's index of AGEs cumulant was 0.440, and the corresponding AGEs cumulant value was 77.65. The corresponding sensitivity and specificity were 0.731 and 0.709, respectively. Furthermore, the maximum Youden's index of neuropathy risk score was 0.385, and the corresponding neuropathy risk score was 66.25. The corresponding sensitivity and the specificity were 0.676 and 0.709, respectively.
The cumulative amount of skin AGEs can be used as the diagnostic index and the prediction and evaluation index of DPN severity. Moreover, the diabetic peripheral neuropathy risk score can predict the risk of DPN in patients with T2DM.

皮肤组织中晚期糖基化终产物(AGEs)的积累可以通过 AGE 阅读器进行测量。在这里,我们评估了 AGEs 值与 2 型糖尿病周围神经病变(DPN)发展之间的相关性。
通过电子系统收集了 560 例 T2DM 患者的基本临床信息。通过非侵入性光学信号检测仪 AGE 阅读器测量 AGEs 和糖尿病并发症风险评分。根据 Dyck 标准,所有参与者被分为 4 组:0 级(非 DPN 组)、1 级(早期组)、2 级(中期组)和 3 级(晚期组)。使用 Pearson 相关分析和 Spearman 相关分析评估 AGEs 与其他指标之间的相关性。通过 ROC 曲线评估糖基化产物的敏感性和特异性。
随着 DPN 严重程度的增加,累积的 AGEs 呈上升趋势。在 DPN 0 级、1 级、2 级和 3 级之间,AGEs 差异显著(P=0.000),1 级和 3 级之间,AGEs 差异显著(P=0.000)。DPN 风险评分在 0 级、1 级、2 级和 3 级之间,1 级、2 级和 3 级之间,2 级和 3 级之间差异显著(P<0.01 或 P<0.05)。AGEs 与年龄、血尿酸、病程、收缩压、糖尿病四大并发症风险评分、肾功能指标(血肌酐、胱抑素 C、同型半胱氨酸、尿白蛋白与肌酐比值、尿微量白蛋白、α-微球蛋白、尿转铁蛋白、尿免疫球蛋白)、炎症指标(白细胞计数、中性粒细胞计数、中性粒细胞与淋巴细胞比值、C 反应蛋白)呈正相关,与 BMI、空腹胰岛素、餐后 1-3 小时胰岛素、淋巴细胞计数、HOMA 胰岛素抵抗指数和估计肾小球滤过率呈负相关。AGEs 累积量和神经病变风险评分曲线下面积分别为 0.769 和 0.743,置信区间分别为(71.2-82.6%)和(68.8-79.9%)。AGEs 累积量的最大 Youden 指数为 0.440,对应的 AGEs 累积量值为 77.65。对应的灵敏度和特异性分别为 0.731 和 0.709。此外,神经病变风险评分的最大 Youden 指数为 0.385,对应的神经病变风险评分为 66.25。对应的灵敏度和特异性分别为 0.676 和 0.709。
皮肤 AGEs 的累积量可作为 DPN 严重程度的诊断指标和预测及评估指标。此外,糖尿病周围神经病变风险评分可预测 T2DM 患者 DPN 的风险。