Department of Radiation, Medicine, University of Kentucky, Lexington, Kentucky, USA.
J Appl Clin Med Phys. 2022 May;23(5):e13608. doi: 10.1002/acm2.13608. Epub 2022 Apr 21.
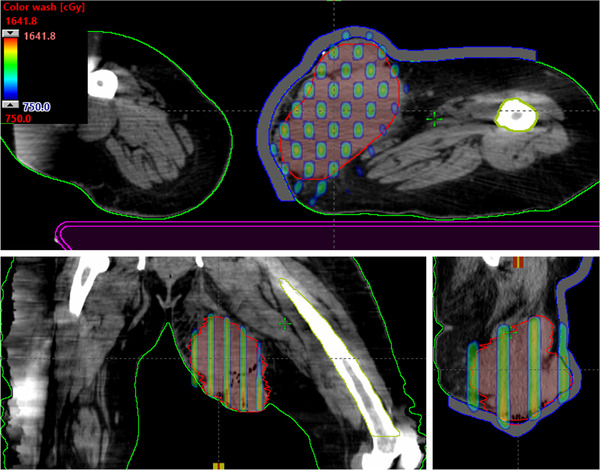
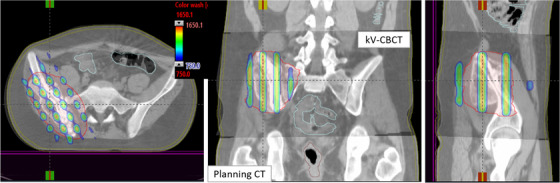
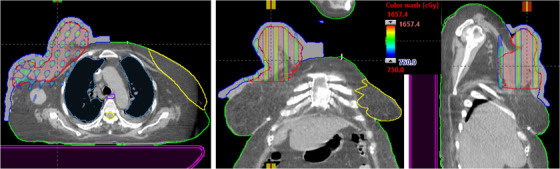
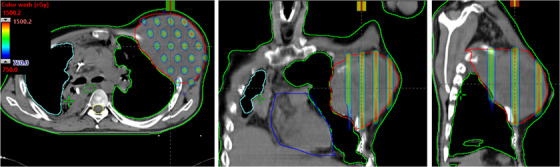
For fast, safe, and effective management of large and bulky (≥8 cm) non-resectable tumors, we have developed a conebeam CT-guided three-dimensional (3D)-conformal MLC-based spatially fractionated radiation therapy (SFRT) treatment. Using an in-house MLC-fitting algorithm, Millennium 120 leaves were fitted to the gross tumor volume (GTV) generating 1-cm diameter holes at 2-cm center-to-center distance at isocenter. SFRT plans of 15 Gy were generated using four to six coplanar crossfire gantry angles 60° apart with a 90° collimator, differentially weighted with 6- or 10-MV beams. A dose was calculated using AcurosXB algorithm, generating sieve-like dose channels without post-processing the physician-drawn GTV contour within an hour of CT simulation allowing for the same day treatment. In total, 50 extracranial patients have been planned and treated using this method, comprising multiple treatment sites. This novel MLC-fitting algorithm provided excellent dose parameters with mean GTV (V7.5 Gy) and mean GTV doses of 53.2% and 7.9 Gy, respectively, for 15 Gy plans. Average peak-to-valley dose ratio was 3.2. Mean beam-on time was 3.32 min, and treatment time, including patient setup and CBCT to beam-off, was within 15 min. Average 3D couch correction from original skin-markers was <1.0 cm. 3D MLC-based SFRT plans enhanced target dose for bulky masses, including deep-seated large tumors while protecting skin and adjacent critical organs. Additionally, it provides the same day, safe, effective, and convenient treatment by eliminating the risk to therapists and patients from heavy gantry-mounted physical GRID-block-we recommend other centers to use this simple and clinically useful method. This rapid SFRT planning technique is easily adoptable in any radiation oncology clinic by eliminating the need for plan optimization and patient-specific quality assurance times while providing dosimetry information in the treatment planning system. This potentially allows for dose-escalation to deep-seated masses to debulk unresectable large tumors providing an option for neoadjuvant treatment. An outcome study of clinical trial is underway.
为了快速、安全、有效地治疗大体积(≥8cm)且无法切除的肿瘤,我们开发了一种基于锥形束 CT 引导的三维(3D)适形多叶准直器(MLC)空间分割放疗(SFRT)治疗方法。使用内部 MLC 拟合算法,将 Millennium 120 叶片拟合到大体肿瘤体积(GTV)上,在等中心处以 2cm 的中心到中心距离生成 1cm 直径的孔。使用四个到六个共面交叉射束机架角度,每个角度相隔 60°,90°准直器,用 6 或 10MV 射线进行不同权重的 15GySFRT 计划。使用 AcurosXB 算法计算剂量,在 CT 模拟后 1 小时内无需对医生勾画的 GTV 轮廓进行后处理,即可生成筛状剂量通道,从而实现当天治疗。共有 50 例颅外患者采用该方法进行了计划和治疗,包括多个治疗部位。这种新型 MLC 拟合算法提供了出色的剂量参数,对于 15Gy 计划,GTV(V7.5Gy)和 GTV 平均剂量分别为 53.2%和 7.9Gy。平均峰谷剂量比为 3.2。平均照射时间为 3.32 分钟,包括患者摆位和从 CBCT 到射束关闭,总时间在 15 分钟以内。从原始皮肤标记到 3D 治疗床的平均校正<1.0cm。基于 3D MLC 的 SFRT 计划提高了大体积肿块的靶区剂量,包括深部大肿瘤,同时保护皮肤和相邻的关键器官。此外,它通过消除治疗师和患者对重型龙门物理栅格阻挡的风险,提供了当天、安全、有效和便捷的治疗,我们建议其他中心使用这种简单且临床有用的方法。这种快速的 SFRT 计划技术可以在任何放射肿瘤学诊所中轻松采用,无需进行计划优化和患者特定的质量保证时间,同时在治疗计划系统中提供剂量学信息。这可能允许对深部肿块进行剂量递增,以缩小无法切除的大肿瘤,为新辅助治疗提供一种选择。一项临床试验的结果研究正在进行中。