Department of Infectious Diseases, The First Affiliated Hospital of Nanchang University, No. 17 Yongwai Street, Donghu District, Nanchang, China.
BMC Gastroenterol. 2022 Apr 21;22(1):196. doi: 10.1186/s12876-022-02263-4.
Recent studies have demonstrated the presence of associations between metabolic syndrome and the onset of nonalcoholic fatty liver disease (NAFLD). Metabolic syndrome, in turn, has been found to be linked to high serum uric acid to HDL-cholesterol ratios (UHR). However, the relationship between UHR values and the occurrence of NAFLD in non-obese individuals remains unknown. The present study aimed to examine the possible correlation between UHR values and NAFLD onset among a non-obese Chinese population without dyslipidemia, as well as comparing the predictive value of UHR versus other NAFLD onset predictors.
A total of 9837 non-obese patients, with normal blood lipid levels, were included in a 5-year retrospective cohort study, and the onset of NAFLD in these patients was diagnosed by liver ultrasound.
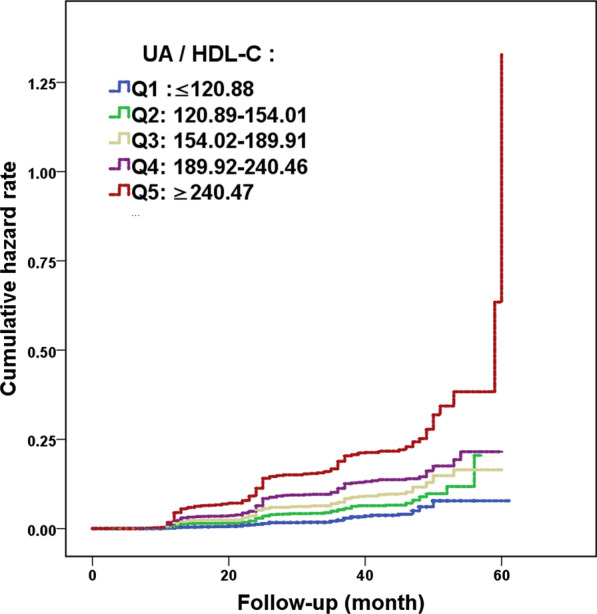
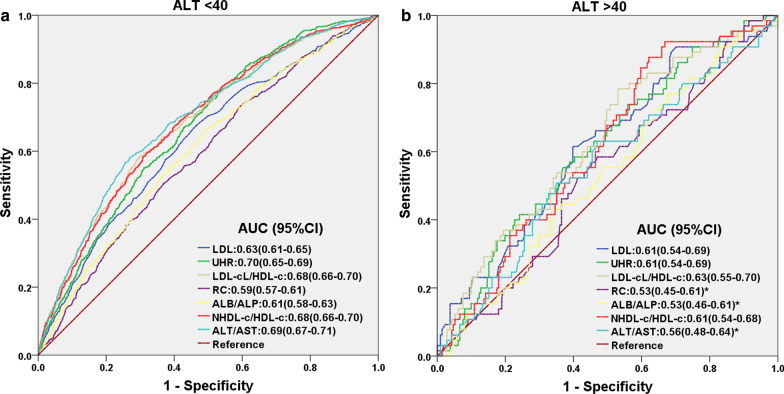
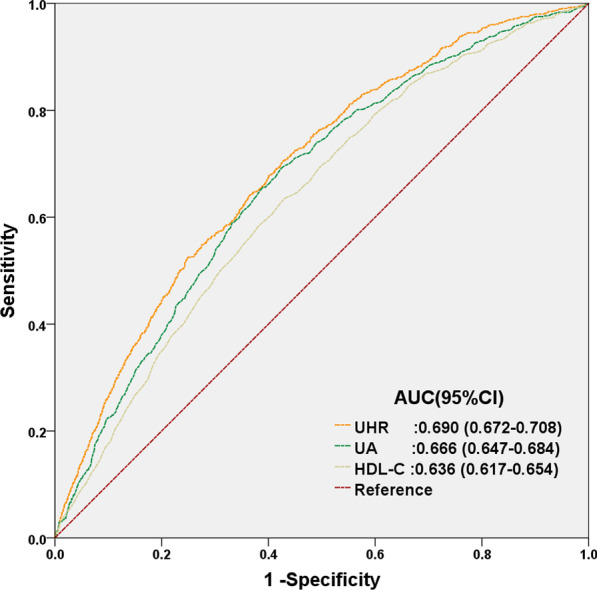
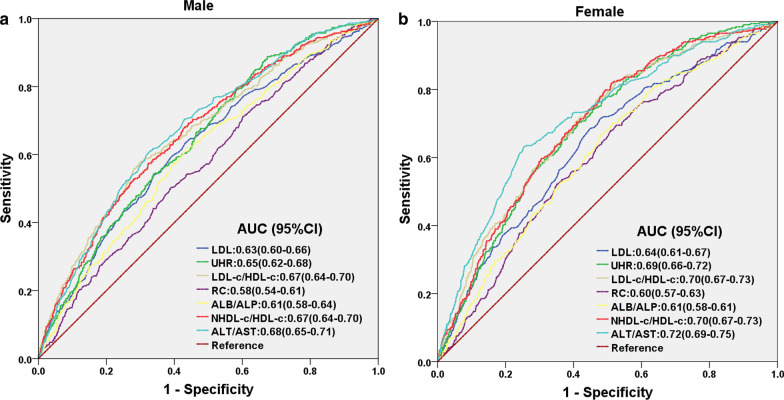
Out of the 9837 patients, 855 were diagnosed with NAFLD during the 5-year follow-up period, for an overall total prevalence of 8.7% at the end of the study period. Across quintiles 1, 2, 3, 4 and 5 of UHR (respectively, ratios of ≤ 120.88, 120.89-154.01, 154.02-189.91, 189.92-240.46, and ≥ 240.47), the prevalence of NAFLD among the patients increased from 2.4%, 5%, 7.9%, 10.3%, and 17.8%, respectively. After adjustments for age, gender, liver and kidney functional markers, as well as metabolic indicators, multivariate Cox proportional hazard regression analysis demonstrated that the hazard ratio (HR) was the highest in quintile 5, at 1.76 (1.12-2.75), and the lowest in quintile 1. The area under the curve (AUC) for UHR (0.690) was higher than that for serum uric acid (UA, 0.666) and HDL-C (0.636), suggesting the predictive ability of UHR for NAFLD onset was better than either alone. This finding was further supported by the presence of an independent association between UHR and NAFLD, even within the normal range of UA and HDL-C; the HR (95% confidence interval, CI) for NAFLD was 1.002 (1.000-1.004). Compared with other significant predictors, AUC for UHR (0.67) was similar to that of low-density lipoprotein cholesterol (LDL-C)/high-density lipoprotein cholesterol (HDL-C, 0.68), non-high-density lipoprotein cholesterol (NHDL-C)/HDL-C (0.68) and alanine aminotransferase (ALT)/aspartate aminotransferase (AST) ratios (0.7), and was higher than that of LDL-C (0.63), remnant cholesterol (RC,0.59), and albumin (ALB)/alkaline phosphatase (ALP) ratio (0.61). The sensitivity of UHR (71%) was the highest among all indicators. In the subgroup with ALT < 40U/L, the AUC for UHR was 0.70, which was the highest among all predictors; among ALT > 40U/L, UHR was able to predict the occurrence of NAFLD (AUC = 0.61, p = 0.007), which was not the case for RC (P = 0.441), ALB/ALP (P = 0.419), and ALT/AST (P = 0.159).
UHR serve as an inexpensive and reliable predictor of NAFLD onset in non-obese Chinese people with normal blood lipid levels, allowing for identification of individuals at high risk for NAFLD.
最近的研究表明,代谢综合征与非酒精性脂肪性肝病(NAFLD)的发生之间存在关联。反过来,高血清尿酸与高密度脂蛋白胆固醇比值(UHR)也与代谢综合征有关。然而,在非肥胖个体中,UHR 值与 NAFLD 发生之间的关系尚不清楚。本研究旨在探讨非肥胖、血脂正常的中国人群中 UHR 值与 NAFLD 发病之间的可能相关性,并比较 UHR 与其他 NAFLD 发病预测因子的预测价值。
共纳入 9837 例非肥胖患者,进行了一项为期 5 年的回顾性队列研究,这些患者的 NAFLD 发病由肝脏超声诊断。
在 9837 例患者中,5 年随访期间有 855 例被诊断为 NAFLD,研究结束时总体患病率为 8.7%。在 UHR(比值分别为≤120.88、120.89-154.01、154.02-189.91、189.92-240.46 和≥240.47)的五分位数 1、2、3、4 和 5 中,患者的 NAFLD 患病率分别为 2.4%、5%、7.9%、10.3%和 17.8%。在校正年龄、性别、肝肾功能标志物以及代谢指标后,多变量 Cox 比例风险回归分析表明,第 5 分位数的风险比(HR)最高,为 1.76(1.12-2.75),第 1 分位数最低。UHR(0.690)的曲线下面积(AUC)高于尿酸(UA,0.666)和高密度脂蛋白胆固醇(HDL-C,0.636),表明 UHR 对 NAFLD 发病的预测能力优于单独使用任何一项指标。即使在 UA 和 HDL-C 正常范围内,UHR 与 NAFLD 之间仍存在独立关联,进一步支持了这一发现;NAFLD 的 HR(95%置信区间,CI)为 1.002(1.000-1.004)。与其他显著预测因子相比,UHR 的 AUC(0.67)与低密度脂蛋白胆固醇(LDL-C)/高密度脂蛋白胆固醇(HDL-C,0.68)、非高密度脂蛋白胆固醇(NHDL-C)/高密度脂蛋白胆固醇(HDL-C,0.68)和丙氨酸氨基转移酶(ALT)/天冬氨酸氨基转移酶(AST)比值(0.7)相似,高于 LDL-C(0.63)、残余胆固醇(RC,0.59)和白蛋白(ALB)/碱性磷酸酶(ALP)比值(0.61)。UHR 的灵敏度(71%)在所有指标中最高。在 ALT<40U/L 的亚组中,UHR 的 AUC 为 0.70,在所有预测因子中最高;在 ALT>40U/L 时,UHR 能够预测 NAFLD 的发生(AUC=0.61,p=0.007),而 RC(P=0.441)、ALB/ALP(P=0.419)和 ALT/AST(P=0.159)则不行。
UHR 是血脂正常的非肥胖中国人 NAFLD 发病的一种廉价且可靠的预测因子,可以识别出发生 NAFLD 的高危人群。