Fleischmann Maximilian, Diefenhardt Markus, Nicolas Adele M, Rödel Franz, Ghadimi Michael, Hofheinz Ralf-Dieter, Greten Florian R, Rödel Claus, Fokas Emmanouil
Department of Radiation Oncology, University Hospital Johann Wolfgang Goethe University, 60590 Frankfurt, Germany.
Institute for Tumor Biology and Experimental Therapy, Georg-Speyer-Haus (GSH), 60596 Frankfurt/Main, Germany.
Clin Transl Radiat Oncol. 2022 Apr 6;34:99-106. doi: 10.1016/j.ctro.2022.04.003. eCollection 2022 May.
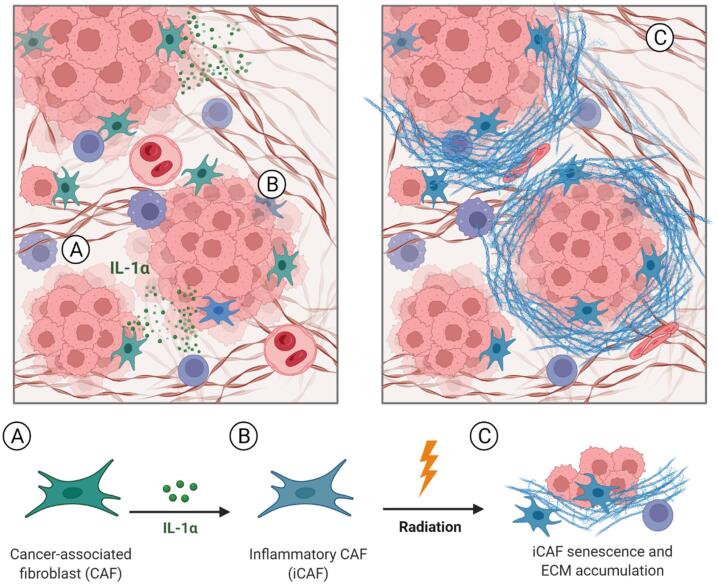
Recent advances in the treatment algorithm of locally advanced rectal cancer (LARC) have significantly improved complete response (CR) rates and disease-free survival (DFS), but therapy resistance, with its substantial impact on outcomes and survival, remains a major challenge. Our group has recently unraveled a critical role of interleukin-1α (IL-1α) signaling in activating inflammatory cancer-associated fibroblasts (iCAFs) and mediating radiation-induced senescence, extracellular matrix (ECM) accumulation, and ultimately therapy resistance. We here summarize the recently initiated ACO/ARO/AIO-21 phase I trial, testing the IL-1 receptor antagonist (IL-1 RA) anakinra in combination with fluoropyrimidine-based chemoradiotherapy (CRT) for advanced rectal cancer.
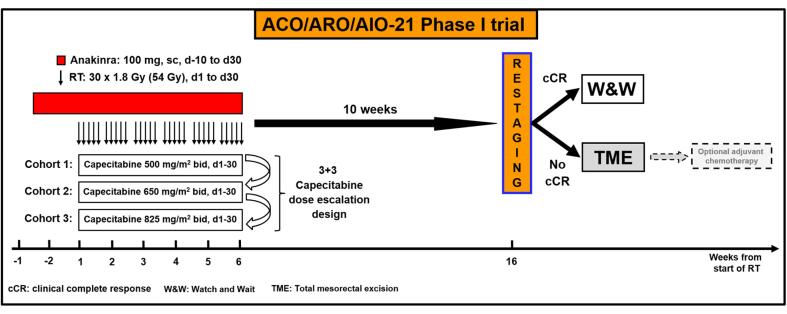
METHODS/DESIGN: The ACO/ARO/AIO-21 is an investigator-driven, prospective, open-labeled phase I drug-repurposing trial assessing the maximum tolerated dose (MTD) of capecitabine administered concurrently to standard preoperative radiotherapy (45 Gy in 25 fractions followed by 9 Gy boost in 5 fractions) in combination with fixed doses of the IL1-RA anakinra (100 mg, days -10 to 30). Capecitabine will be administered using a 3 + 3 dose-escalation design (500 mg/m bid; 650 mg/m bid; 825 mg/m bid, respectively) from day 1 to day 30. Response assessment including digital rectal examination (DRE), endoscopy and pelvic magnetic resonance imaging (MRI) is scheduled 10 weeks after completion of CRT. For patients achieving clinical complete response (cCR), primary non-operative management is provided. In case of non-cCR immediate total mesorectal excision (TME) will be performed. Primary endpoint of this phase I trial is the MTD of capecitabine.
Based on extensive preclinical research, the ACO/ARO/AIO-21 phase I trial will assess whether the IL-1RA anakinra can be safely combined with fluoropyrimidine-based CRT in rectal cancer. It will further explore the potential of IL-1 inhibition to overcome therapy resistance and improve response rates. A comprehensive translational research program will expand our understanding from a clinical perspective and may help translate the results into a randomized phase II trial.
局部晚期直肠癌(LARC)治疗方案的最新进展显著提高了完全缓解(CR)率和无病生存期(DFS),但治疗耐药性对治疗结果和生存仍有重大影响,仍是一个主要挑战。我们团队最近揭示了白细胞介素-1α(IL-1α)信号在激活炎性癌症相关成纤维细胞(iCAF)以及介导辐射诱导的衰老、细胞外基质(ECM)积累并最终导致治疗耐药性方面的关键作用。在此,我们总结了最近启动的ACO/ARO/AIO-21 I期试验,该试验测试了IL-1受体拮抗剂(IL-1 RA)阿那白滞素联合氟嘧啶类同步放化疗(CRT)用于晚期直肠癌的疗效。
方法/设计:ACO/ARO/AIO-21是一项由研究者发起的前瞻性、开放标签的I期药物再利用试验,评估在标准术前放疗(25次分割给予45 Gy,随后5次分割给予9 Gy推量)同时给予卡培他滨的最大耐受剂量(MTD),并联合固定剂量的IL-1 RA阿那白滞素(100 mg,第-10天至第30天)。从第1天至第30天,卡培他滨将采用3+3剂量递增设计(分别为500 mg/m² bid;650 mg/m² bid;825 mg/m² bid)给药。在CRT完成10周后安排包括直肠指检(DRE)、内镜检查和盆腔磁共振成像(MRI)在内的疗效评估。对于达到临床完全缓解(cCR)的患者,给予主要的非手术治疗。如果未达到cCR,则立即进行全直肠系膜切除术(TME)。该I期试验的主要终点是卡培他滨的MTD。
基于广泛的临床前研究,ACO/ARO/AIO-21 I期试验将评估IL-1 RA阿那白滞素是否能与氟嘧啶类CRT安全联合用于直肠癌治疗。它还将进一步探索IL-1抑制克服治疗耐药性并提高缓解率的潜力。一项全面的转化研究计划将从临床角度扩展我们的认识,并可能有助于将结果转化为随机II期试验。