Kirigaya Jin, Iwahashi Noriaki, Tanaka Reiko, Inayama Yoshiaki, Takeuchi Ichiro
Advanced Critical Care and Emergency Center, Yokohama City University Medical Center, Yokohama, JPN.
Division of Cardiology, Yokohama City University Medical Center, Yokohama, JPN.
Cureus. 2022 Mar 18;14(3):e23287. doi: 10.7759/cureus.23287. eCollection 2022 Mar.
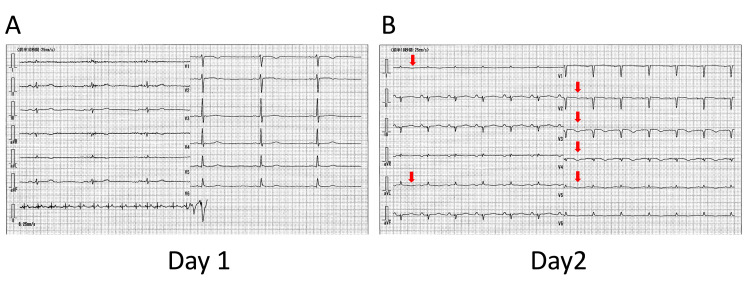
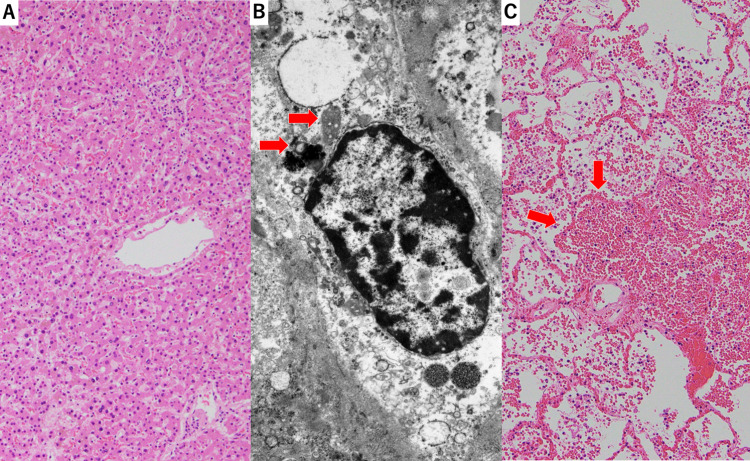
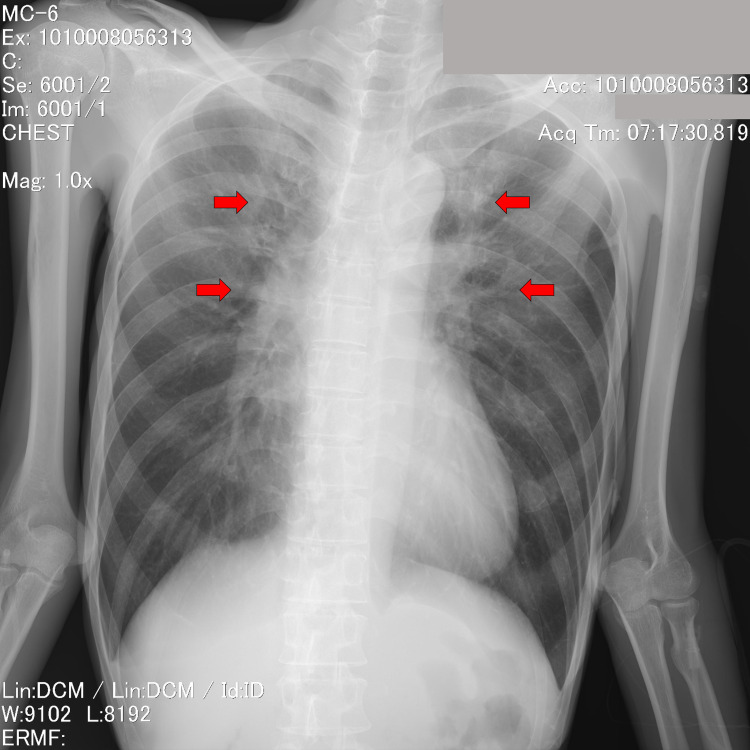
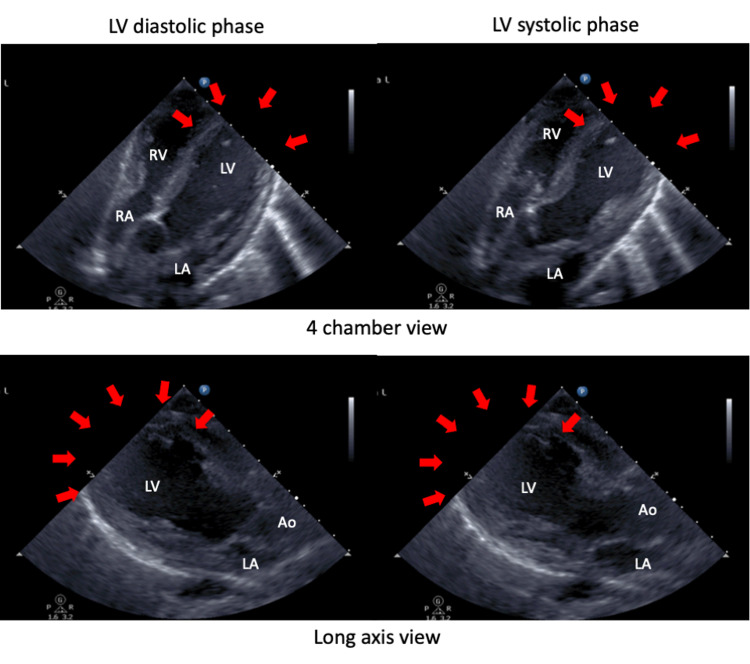
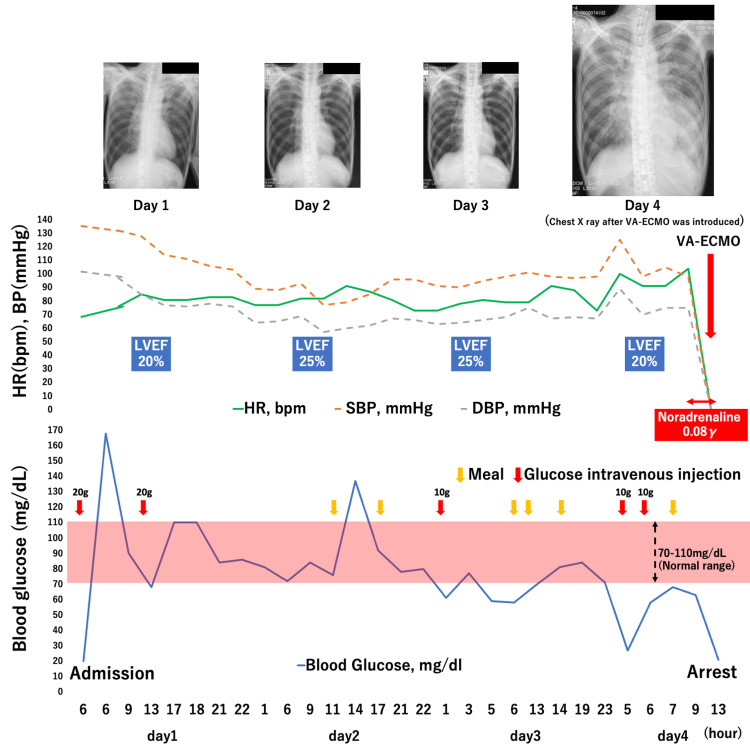
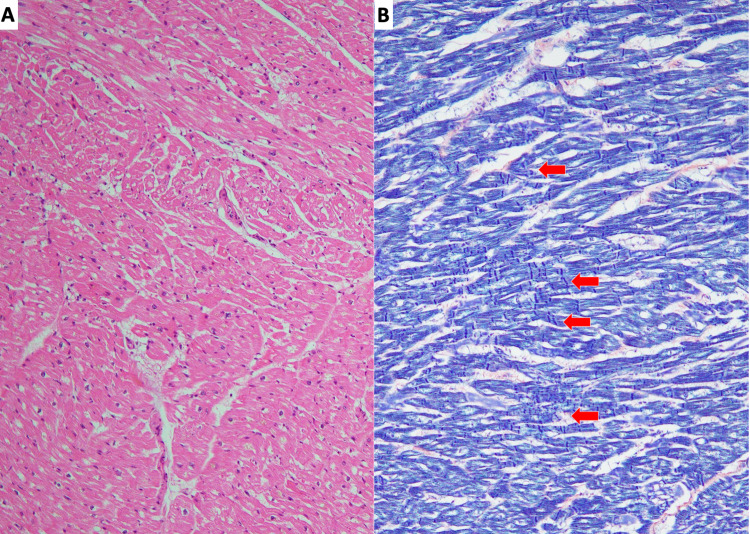
A 56-year-old, severely malnourished man presented with loss of consciousness due to hypoglycemia. Echocardiography revealed left ventricular apical ballooning, indicating takotsubo cardiomyopathy. Although his caloric intake was gradually increased to avoid refeeding syndrome, hypoglycemia was refractory, and repetitive glucose administration was required. On day 4 of admission, he developed severe refractory hypoglycemia with a progressive decrease in blood pressure. Consequently, pulseless ventricular tachycardia followed by pulseless electrical activity developed. Although venoarterial extracorporeal membrane oxygenation was introduced, the patient did not respond to the treatment and died. Autopsy revealed myocardial degeneration and contraction-band necrosis, indicative of takotsubo cardiomyopathy. No coronary stenosis was observed. The liver showed moderate hepatocyte atrophy and autophagosomes, consistent with starvation and not with refeeding syndrome. We speculated that refractory hypoglycemia induced extreme catecholamine secretion, which led to severe complications of takotsubo cardiomyopathy, such as fatal arrhythmia and extremely low cardiac output. Early recognition of these critically ill patients and timely therapeutic interventions, including strict glycemic control and adequate caloric intake, may improve patient outcomes.
一名56岁、严重营养不良的男性因低血糖导致意识丧失。超声心动图显示左心室心尖部气球样改变,提示应激性心肌病。尽管逐渐增加其热量摄入以避免再喂养综合征,但低血糖难以纠正,需要反复给予葡萄糖。入院第4天,他出现严重难治性低血糖,血压逐渐下降。随后出现无脉性室性心动过速,继之出现无脉性电活动。尽管进行了静脉-动脉体外膜肺氧合治疗,但患者对治疗无反应,最终死亡。尸检显示心肌变性和收缩带坏死,提示应激性心肌病。未观察到冠状动脉狭窄。肝脏显示中度肝细胞萎缩和自噬体,符合饥饿表现而非再喂养综合征。我们推测难治性低血糖诱发了极端的儿茶酚胺分泌,进而导致应激性心肌病的严重并发症,如致命性心律失常和极低的心输出量。早期识别这些危重症患者并及时进行治疗干预,包括严格控制血糖和给予充足的热量摄入,可能会改善患者的预后。