Schwander Bjoern, Feldstein Josh, Sulo Suela, Gonzalez Luis, ElShishiney Galal, Hassany Mohamed
AHEAD GmbH-Agency for Health Economic Assessment and Dissemination, Bietigheim-Bissingen, Germany.
CAVA, LLC, 145 University Drive, Suite 2660, Amherst, MA, 01004, USA.
Infect Dis Ther. 2022 Jun;11(3):1193-1203. doi: 10.1007/s40121-022-00631-x. Epub 2022 Apr 22.
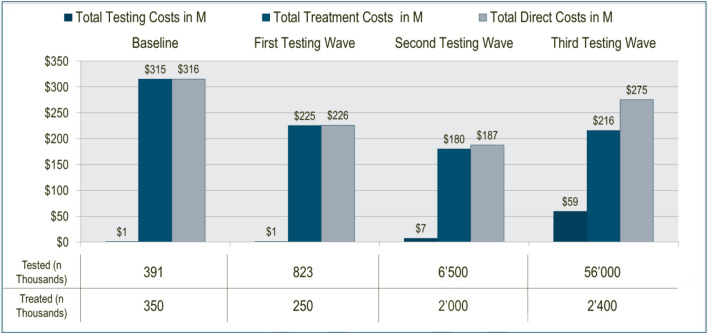
Hepatitis C virus (HCV) is a global public health crisis. Egypt presents the highest HCV global prevalence. Recently, three different HCV screening/testing/therapy programs were implemented: In 2014 (wave 1), major decisions on HCV therapy were enacted, accompanied by a 99% discount for the HCV therapy sofosbuvir. In 2016 (wave 2), a first testing program was launched to identify patients for free treatment. In 2018 (wave 3), population-wide screening was conducted using a WHO-prequalified finger prick rapid diagnostic test (RDT) to identify/treat all Egyptians with HCV. The financial advantages of HCV screening programs (wave 1-3 results) were estimated vs a baseline period of limited Egyptian HCV testing/therapeutic intervention (2008-2014).
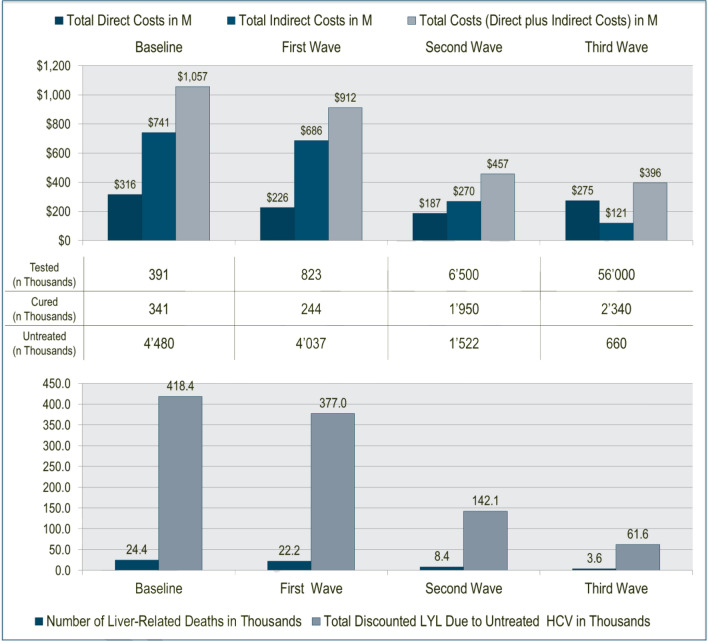
Using published evidence and model-based estimates from real-world data, we evaluated the direct costs of the different HCV programs, accompanied by a conservative simulation of major HCV health consequences (i.e., liver-related deaths/life years lost) and related indirect costs. Total economic consequences of each HCV program were compared to each other and baseline from a societal perspective. Future costs and health effects were discounted by 3.5% per year.
Discounted total costs (in US dollars) were $1,057 billion (baseline), $913 million (wave 1), $457 million (wave 2), and $396 million (wave 3). Discounted HCV-related life years lost were 418,000 (baseline), 377,000 (wave 1), 142,000 (wave 2), and 62,000 (wave 3). With each successive Egyptian HCV screening/testing/therapy wave, total costs and HCV-related mortality were reduced.
Use of the community-applied, WHO-prequalified RDT was the most dominant approach to cost-effectiveness. These results provide rationale for worldwide scalability of similar HCV elimination programs.
丙型肝炎病毒(HCV)是一场全球公共卫生危机。埃及是全球丙型肝炎病毒感染率最高的国家。最近,实施了三种不同的丙型肝炎病毒筛查/检测/治疗方案:2014年(第1波),颁布了关于丙型肝炎病毒治疗的重大决策,同时丙型肝炎病毒治疗药物索磷布韦享受99%的折扣。2016年(第2波),启动了首个检测方案,以确定可接受免费治疗的患者。2018年(第3波),使用世界卫生组织预认证的手指采血快速诊断检测(RDT)对全体人群进行筛查,以识别/治疗所有感染丙型肝炎病毒的埃及人。与埃及丙型肝炎病毒检测/治疗干预有限的基线期(2008 - 2014年)相比,评估了丙型肝炎病毒筛查方案(第1 - 3波结果)的经济优势。
利用已发表的证据和基于实际数据的模型估计,我们评估了不同丙型肝炎病毒方案的直接成本,并对主要丙型肝炎病毒健康后果(即肝脏相关死亡/生命年损失)及相关间接成本进行了保守模拟。从社会角度比较了每个丙型肝炎病毒方案的总体经济后果及其与基线的差异。未来成本和健康影响按每年3.5%进行贴现。
贴现后的总成本(以美元计)分别为:1057亿美元(基线)、9.13亿美元(第1波)、4.57亿美元(第2波)和3.96亿美元(第3波)。贴现后的丙型肝炎病毒相关生命年损失分别为:41.8万(基线)、37.7万(第1波)、14.2万(第2波)和6.2万(第3波)。随着埃及丙型肝炎病毒筛查/检测/治疗的每一波推进,总成本和丙型肝炎病毒相关死亡率均有所降低。
使用社区应用的、世界卫生组织预认证的快速诊断检测是最具成本效益的主要方法。这些结果为类似的丙型肝炎病毒消除计划在全球范围内的推广提供了依据。