Vandevelde Arne, Devreese Katrien M J
Department of Diagnostic Sciences, Ghent University, 9000 Gent, Belgium.
Coagulation Laboratory, Ghent University Hospital, 9000 Gent, Belgium.
J Clin Med. 2022 Apr 13;11(8):2164. doi: 10.3390/jcm11082164.
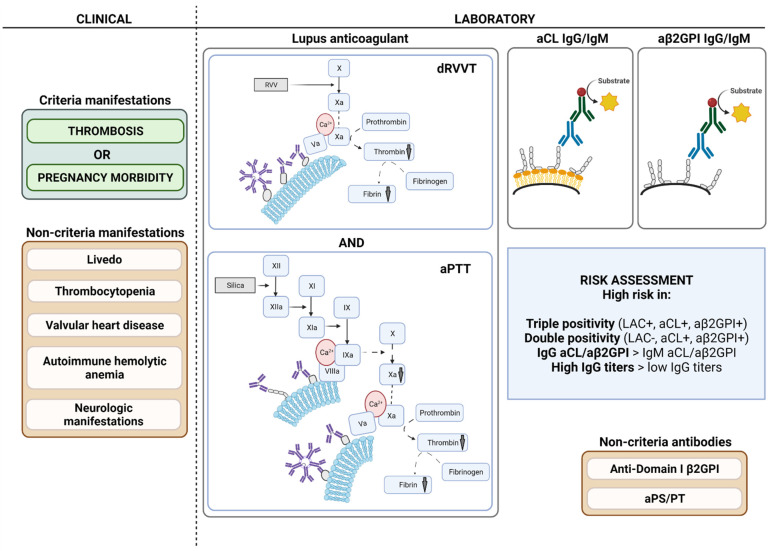
Diagnosis of antiphospholipid syndrome (APS) requires the presence of a clinical criterion (thrombosis and/or pregnancy morbidity), combined with persistently circulating antiphospholipid antibodies (aPL). Currently, laboratory criteria aPL consist of lupus anticoagulant (LAC), anticardiolipin antibodies (aCL) IgG/IgM, and anti-β2 glycoprotein I antibodies (aβ2GPI) IgG/IgM. Diagnosis and risk stratification of APS are complex and efforts to standardize and optimize laboratory tests have been ongoing since the initial description of the syndrome. LAC detection is based on functional coagulation assays, while aCL and aβ2GPI are measured with immunological solid-phase assays. LAC assays are especially prone to interference by anticoagulation therapy, but strategies to circumvent this interference are promising. Alternative techniques such as thrombin generation for LAC detection and to estimate LAC pathogenicity have been suggested, but are not applicable yet in routine setting. For aCL and aβ2GPI, a lot of different assays and detection techniques such as enzyme-linked immunosorbent and chemiluminescent assays are available. Furthermore, a lack of universal calibrators or standards results in high variability between the different solid-phase assays. Other non-criteria aPL such as anti-domain I β2 glycoprotein I and antiphosphatidylserine/prothrombin antibodies have been suggested for risk stratification purposes in APS, while their added value to diagnostic criteria seems limited. In this review, we will describe laboratory assays for diagnostic and risk evaluation in APS, integrating applicable guidelines and classification criteria. Current insights and hindrances are addressed with respect to both laboratory and clinical implications.
抗磷脂综合征(APS)的诊断需要具备临床标准(血栓形成和/或妊娠并发症),并伴有持续循环的抗磷脂抗体(aPL)。目前,实验室诊断标准中的aPL包括狼疮抗凝物(LAC)、抗心磷脂抗体(aCL)IgG/IgM以及抗β2糖蛋白I抗体(aβ2GPI)IgG/IgM。APS的诊断和风险分层较为复杂,自该综合征首次被描述以来,一直在努力规范和优化实验室检测。LAC检测基于功能性凝血试验,而aCL和aβ2GPI则通过免疫固相试验进行检测。LAC试验特别容易受到抗凝治疗的干扰,但规避这种干扰的策略很有前景。已经有人提出了替代技术,如用于LAC检测和评估LAC致病性的凝血酶生成试验,但尚未应用于常规检测。对于aCL和aβ2GPI,有许多不同的试验和检测技术,如酶联免疫吸附试验和化学发光试验。此外,缺乏通用校准物或标准导致不同固相试验之间的变异性很大。其他非标准aPL,如抗结构域Iβ2糖蛋白I和抗磷脂酰丝氨酸/凝血酶原抗体,已被建议用于APS的风险分层,但其对诊断标准的附加价值似乎有限。在这篇综述中,我们将描述用于APS诊断和风险评估的实验室检测方法,并整合适用的指南和分类标准。针对实验室和临床意义方面,阐述了当前的见解和障碍。