Eck Institute for Global Health, University of Notre Dame, Notre Dame, IN, USA.
Palliative Care Association of Uganda, Kampala, Uganda.
BMC Palliat Care. 2022 Apr 22;21(1):55. doi: 10.1186/s12904-022-00930-7.
The first and most recent nationwide audit of palliative care services in Uganda was conducted in 2009. Since then, Uganda has made great strides in palliative care development, including policy, education, and services implementation. This study provides an overview of the availability of palliative care services in the country and the challenges and gaps in Uganda prior to the global COVID-19 pandemic. This lays the foundation for better understanding the challenges and changes needed to support palliative care development and access in the wake of the pandemic.
We conducted a descriptive quantitative study of secondary data on nationwide morphine distribution, collated a list of accredited facilities, and analyzed key palliative care indicators collected through the mHealth surveillance project present at a subset of accredited facilities. Descriptive statistical analysis involved non-parametric tests using SPSS, mapping geographical distribution of available palliative care services using Geographic Information Systems software, and identification of challenges from the subset of accredited facilities.
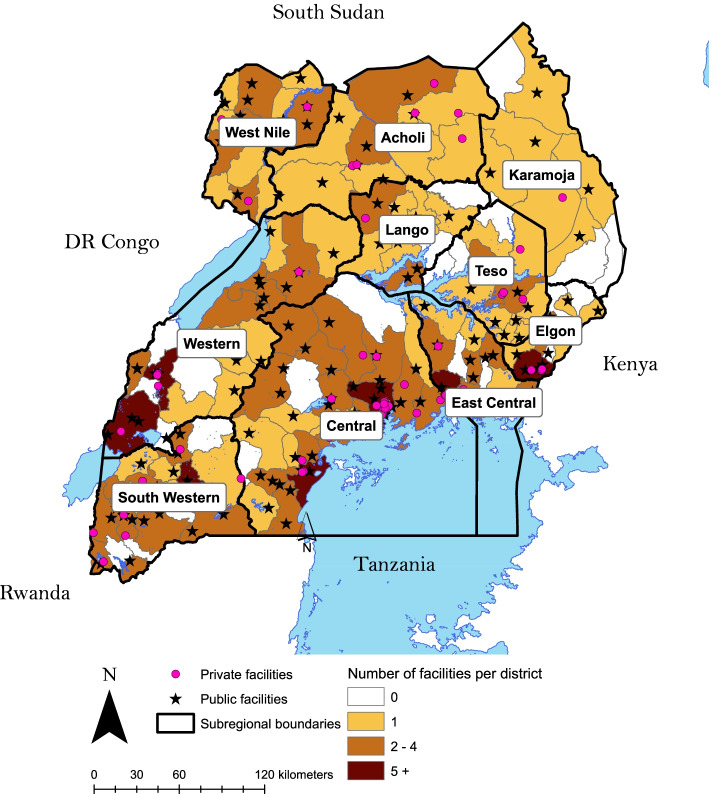
There were 226 accredited palliative care facilities across Uganda's 135 districts in 2020. Thirty districts lacked any accredited palliative care facility. The estimated population coverage was 88.5%. The majority (68.1%) of accredited facilities were public, and private facilities received slightly more pain-relieving morphine. There was an alternating trend in the volumes of morphine delivered to public and private facilities. More than a third of the patients were diagnosed with non-communicable diseases, highlighting their significance alongside cancer and HIV/AIDS as conditions requiring palliative care. Palliative care accredited facilities offered six types of services: outreach, home visits, psychosocial, legal, bereavement, and spiritual support, but only for an average of 7 months a year due to lack of facilitation and transportation.
Palliative care in Uganda developed in quality, volume, and geographic coverage since 2009. The shift in palliative care patients' primary diagnosis from HIV/AIDS to non-communicable diseases marks an important epidemiologic transition. Although accredited facilities are present in most administrative districts, more research is needed to evaluate the actual accessibility of these services. The existing services, both private and public, are limited by the amount of pain-relieving morphine, financial and transport resources. More quality data collected on key palliative care indicators is needed into geographical accessibility of palliative care services, morphine availability trends, and patient diagnoses in order to improve the provision of palliative care in Uganda.
乌干达首次也是最近一次全国性的姑息治疗服务审计于 2009 年进行。自那时以来,乌干达在姑息治疗发展方面取得了长足的进步,包括政策、教育和服务的实施。本研究概述了该国姑息治疗服务的可及性,以及在全球 COVID-19 大流行之前乌干达存在的挑战和差距。这为更好地理解大流行后支持姑息治疗发展和可及性所需的挑战和变化奠定了基础。
我们对全国范围内吗啡分配的二次数据进行了描述性定量研究,整理了认可设施清单,并通过在认可设施中的一部分进行的移动医疗监测项目收集了关键姑息治疗指标进行了分析。描述性统计分析涉及使用 SPSS 进行非参数检验、使用地理信息系统软件绘制可用姑息治疗服务的地理分布,以及从认可设施中的一部分确定挑战。
2020 年,乌干达 135 个区中有 226 个姑息治疗认可设施。30 个区没有任何姑息治疗认可设施。估计人口覆盖率为 88.5%。大多数(68.1%)认可设施为公立,私立设施略多获得缓解疼痛的吗啡。公立和私立设施的吗啡输送量呈交替趋势。超过三分之一的患者被诊断患有非传染性疾病,这凸显了它们与癌症和艾滋病一样,作为需要姑息治疗的疾病的重要性。姑息治疗认可设施提供了六种服务类型:外展、家访、心理社会、法律、丧亲、和精神支持,但由于缺乏便利和交通,每年仅提供平均 7 个月的服务。
自 2009 年以来,乌干达的姑息治疗在质量、数量和地理覆盖范围方面都有所发展。姑息治疗患者的主要诊断从艾滋病病毒/艾滋病转变为非传染性疾病,标志着一个重要的流行病学转变。尽管大多数行政区都有姑息治疗认可设施,但仍需要更多的研究来评估这些服务的实际可及性。现有的私立和公立服务都受到缓解疼痛的吗啡数量、财务和交通资源的限制。为了改善乌干达的姑息治疗提供,需要收集更多关于姑息治疗关键指标的高质量数据,包括姑息治疗服务的地理可及性、吗啡供应趋势以及患者诊断情况。
