Department of Pulmonary Medicine, Inselspital University Hospital Bern, Bern, Switzerland.
Department of Internal Medicine, Hopital cantonal de Fribourg, Fribourg, Switzerland.
BMJ Open Respir Res. 2022 Apr;9(1). doi: 10.1136/bmjresp-2022-001227.
The Clinical Frailty Scale (CFS) is increasingly used for clinical decision making in acute care but little is known about frailty after COVID-19.
To investigate frailty and the CFS for post-COVID-19 follow-up.
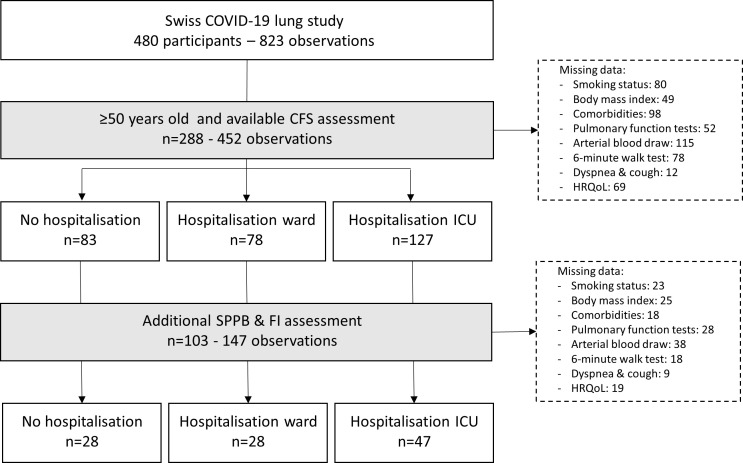
This prospective multicentre cohort study included COVID-19 survivors aged ≥50 years presenting for a follow-up visit ≥3 months after the acute illness. Nine centres retrospectively collected pre-COVID-19 CFS and prospectively CFS at follow-up. Three centres completed the Frailty Index (FI), the short physical performance battery (SPPB), 30 s sit-to-stand test and handgrip strength measurements. Mixed effect logistic regression models accounting for repeated measurements and potential confounders were used to investigate factors associated with post-COVID-19 CFS. Criterion and construct validity were determined by correlating the CFS to other concurrently assessed frailty measurements and measures of respiratory impairment, respectively.
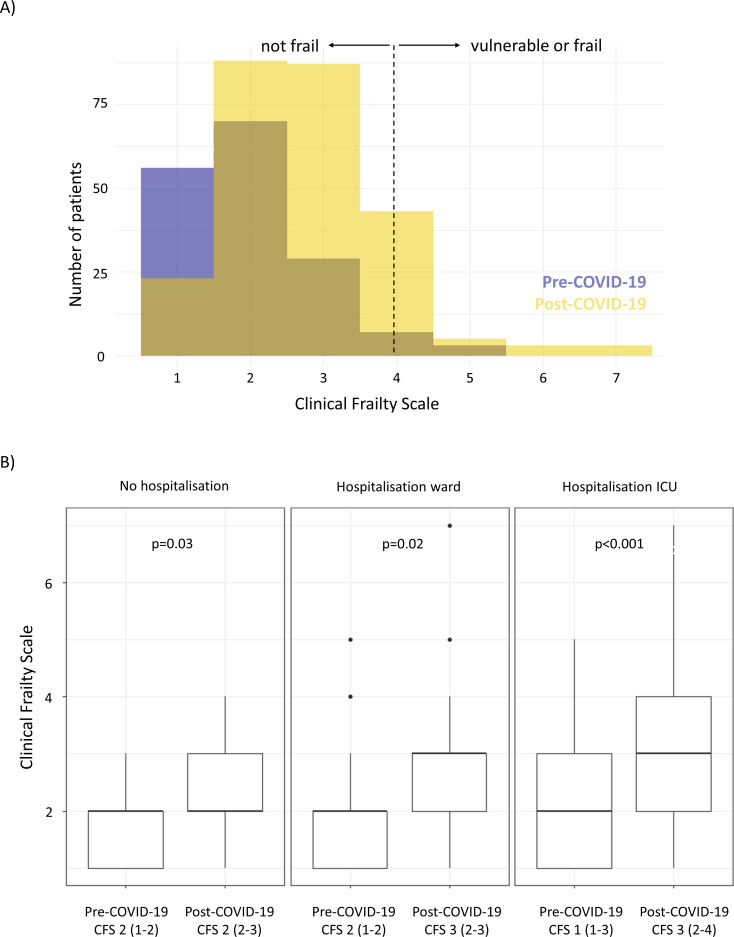
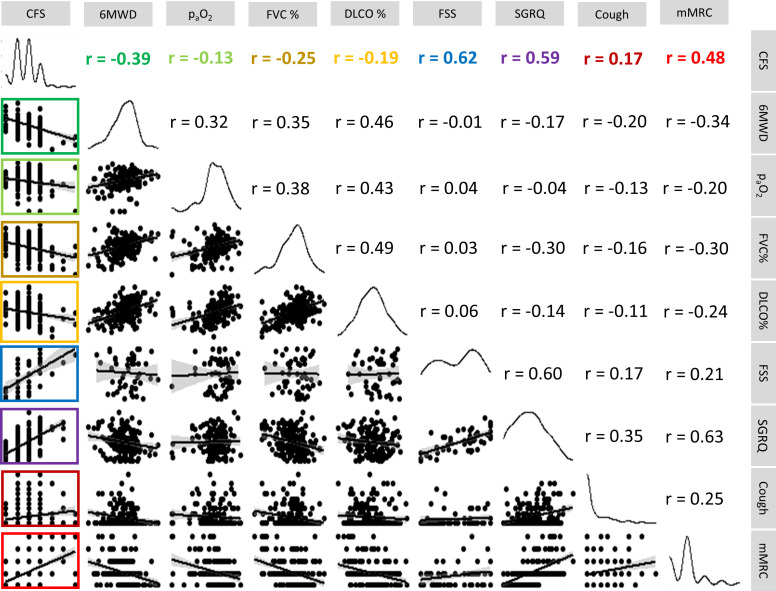
Of the 288 participants 65% were men, mean (SD) age was 65.1 (9) years. Median (IQR) CFS at follow-up was 3 (2-3), 21% were vulnerable or frail (CFS ≥4). The CFS was responsive to change, correlated with the FI (r=0.69, p<0.001), the SPPB score (r=-0.48, p<0.001) (criterion validity) and with the St George's Respiratory Questionnaire score (r=0.59, p<0.001), forced vital capacity %-predicted (r=-0.25, p<0.001), 6 min walk distance (r=-0.39, p<0.001) and modified Medical Research Council (mMRC) (r=0.59, p<0.001). Dyspnoea was significantly associated with a higher odds for vulnerability/frailty (per one mMRC adjusted OR 2.01 (95% CI 1.13 to 3.58), p=0.02).
The CFS significantly increases with COVID-19, and dyspnoea is an important risk factor for post-COVID-19 frailty and should be addressed thoroughly.
临床虚弱量表(CFS)越来越多地用于急性护理中的临床决策,但对于 COVID-19 后的虚弱情况知之甚少。
调查 COVID-19 后的虚弱和 CFS。
本前瞻性多中心队列研究纳入了年龄≥50 岁的 COVID-19 幸存者,他们在急性疾病后≥3 个月就诊进行随访。9 个中心回顾性收集 COVID-19 前的 CFS,并前瞻性收集随访时的 CFS。3 个中心完成了虚弱指数(FI)、短体适能电池测试(SPPB)、30 秒坐立测试和握力测量。采用混合效应逻辑回归模型,考虑重复测量和潜在混杂因素,调查与 COVID-19 后 CFS 相关的因素。通过将 CFS 与同时评估的其他虚弱测量和呼吸受损测量相关联,确定标准和结构效度。
288 名参与者中,65%为男性,平均(SD)年龄为 65.1(9)岁。随访时的 CFS 中位数(IQR)为 3(2-3),21%为脆弱或虚弱(CFS≥4)。CFS 对变化敏感,与 FI(r=0.69,p<0.001)、SPPB 评分(r=-0.48,p<0.001)(标准效度)和圣乔治呼吸问卷评分(r=0.59,p<0.001)、用力肺活量预测值(r=-0.25,p<0.001)、6 分钟步行距离(r=-0.39,p<0.001)和改良医学研究委员会(mMRC)呼吸困难量表(r=0.59,p<0.001)相关。呼吸困难与脆弱/虚弱的可能性增加显著相关(每增加一个 mMRC 调整后的 OR 为 2.01(95%CI 1.13 至 3.58),p=0.02)。
COVID-19 后 CFS 显著增加,呼吸困难是 COVID-19 后虚弱的一个重要危险因素,应彻底处理。