Department of Neuromedicine and Movement Science, Department of Neuromedicine and Movement Science, Faculty of Medicine and Health Science, Trondheim, Norway
Department of Stroke, Clinic of Medicine, St Olavs Hospital Trondheim University Hospital, Trondheim, Norway.
Open Heart. 2022 Apr;9(1). doi: 10.1136/openhrt-2022-001972.
Elevated low-density lipoprotein cholesterol (LDL-C) increases the risk of recurrent cardiovascular disease (CVD) events. We examined use of lipid-lowering therapy (LLT) following ischaemic stroke, and estimated benefits from guideline-based up-titration of LLT.
The Norwegian COgnitive Impairment After STroke (Nor-COAST) study, a multicentre prospective cohort study, collected data on LLT use, dose intensity and LDL-C levels for 462 home-dwelling patients with ischaemic stroke. We used the Secondary Manifestations of Arterial Disease-Reduction of Atherothrombosis for Continued Health (SMART-REACH) model to estimate the expected benefit of up-titrating LLT.
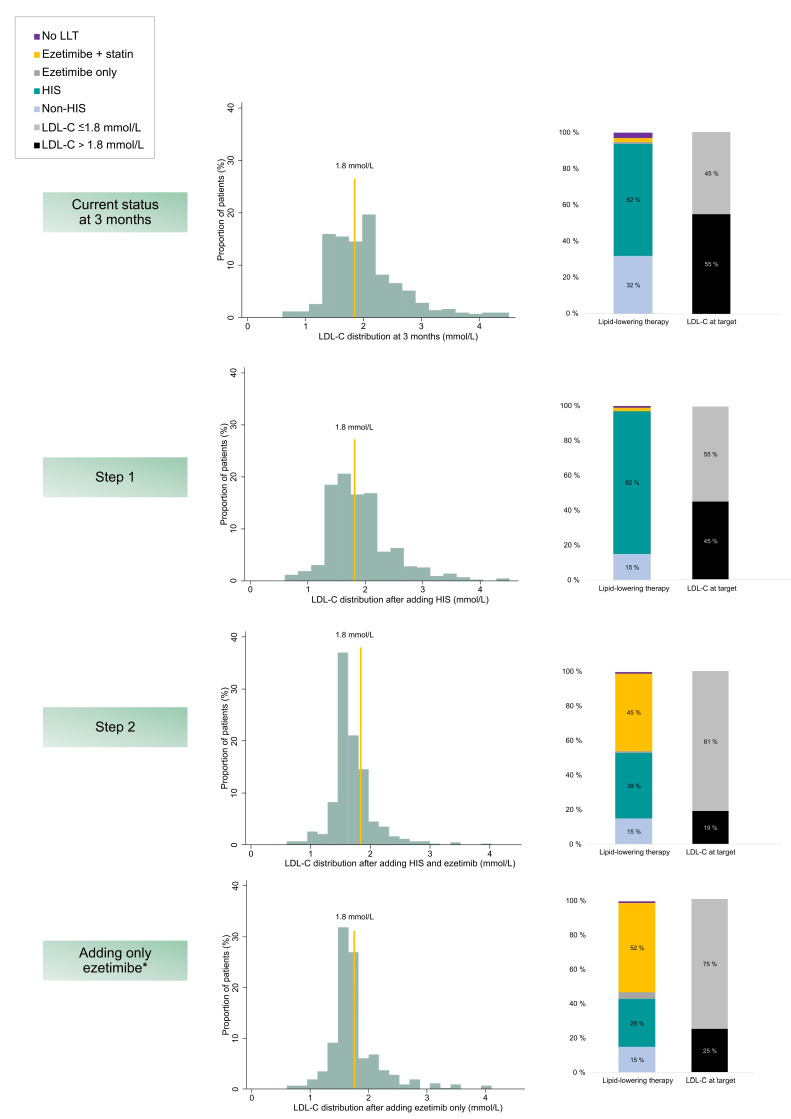
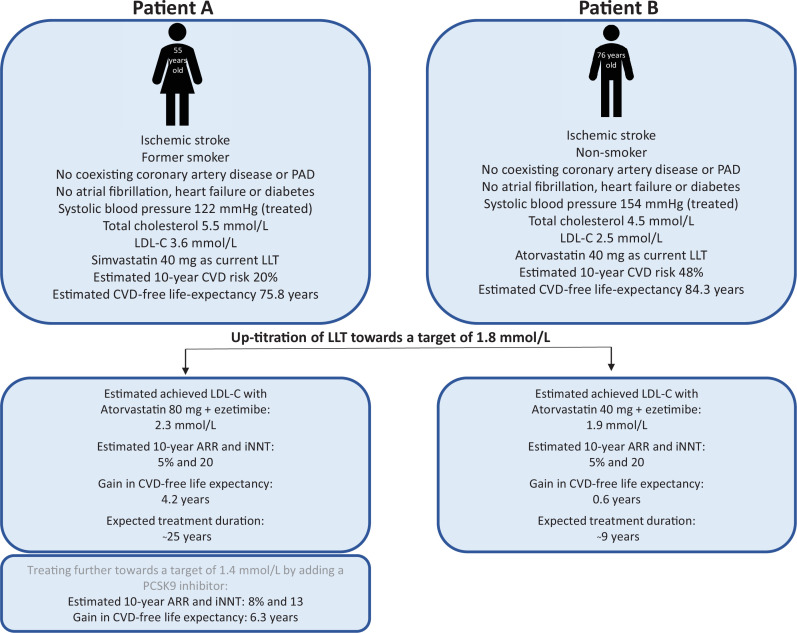
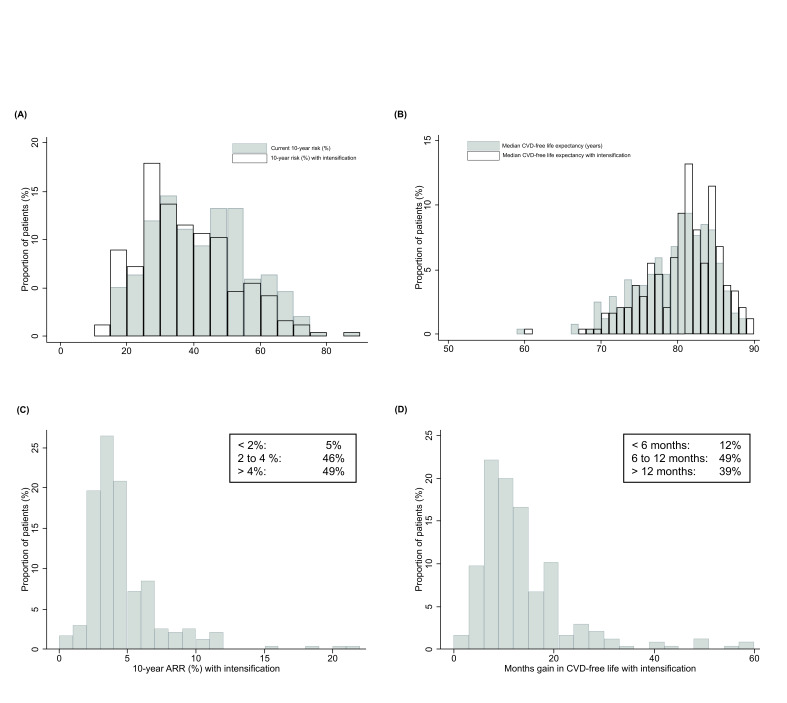
At discharge, 92% received LLT (97% statin monotherapy). Patients with prestroke dementia and cardioembolic stroke aetiology were less likely to receive LLT. Older patients (coefficient -3 mg atorvastatin per 10 years, 95% CI -6 to -0.5) and women (coefficient -5.1 mg atorvastatin, 95% CI -9.2 to -0.9) received lower doses, while individuals with higher baseline LDL-C, ischaemic heart disease and large artery stroke aetiology received higher dose intensity. At 3 months, 45% reached LDL-C ≤1.8 mmol/L, and we estimated that 81% could potentially reach the target with statin and ezetimibe, resulting in median 5 (IQR 0-12) months of CVD-free life gain and median 2% 10-year absolute risk reduction (IQR 0-4) with large interindividual variation.
Potential for optimisation of conventional LLT use exists in patients with ischaemic stroke. Awareness of groups at risk of undertreatment and objective estimates of the individual patient's benefit of intensification can help personalise treatment decisions and reduce residual cholesterol risk.
NCT02650531.
升高的低密度脂蛋白胆固醇(LDL-C)会增加复发性心血管疾病(CVD)事件的风险。我们研究了缺血性中风后使用降脂治疗(LLT)的情况,并估计了基于指南的 LLT 增量滴定的获益。
挪威认知障碍后中风(Nor-COAST)研究是一项多中心前瞻性队列研究,为 462 名居住在家庭中的缺血性中风患者收集了 LLT 使用、剂量强度和 LDL-C 水平的数据。我们使用动脉疾病二级表现-减少动脉粥样硬化血栓形成以维持健康(SMART-REACH)模型来估计增量滴定 LLT 的预期获益。
出院时,92%的患者接受了 LLT(97%为他汀类药物单药治疗)。有中风前痴呆和心源性栓塞性中风病因的患者接受 LLT 的可能性较低。年龄较大的患者(每增加 10 年阿托伐他汀 3 毫克的系数,95%CI-6 至-0.5)和女性(阿托伐他汀 5.1 毫克的系数,95%CI-9.2 至-0.9)接受的剂量较低,而基线 LDL-C 较高、缺血性心脏病和大动脉性中风病因的患者接受的剂量强度较高。在 3 个月时,45%的患者达到 LDL-C≤1.8mmol/L,我们估计 81%的患者可以通过使用他汀类药物和依折麦布达到目标,从而获得中位 5(IQR 0-12)个月的无 CVD 生存获益和中位 2%的 10 年绝对风险降低(IQR 0-4),个体间差异较大。
缺血性中风患者使用常规 LLT 的优化潜力仍然存在。对治疗不足风险的认识和对个体患者强化治疗获益的客观估计,可以帮助个体化治疗决策并降低残留胆固醇风险。
NCT02650531。