Division of Infection, Immunity and Respiratory Medicine, The University of Manchester, Manchester, UK.
Prevention and Early Detection Theme, NIHR Manchester Biomedical Research Centre, Manchester, UK.
Thorax. 2020 Aug;75(8):661-668. doi: 10.1136/thoraxjnl-2020-214626. Epub 2020 Jul 6.
Low-dose CT (LDCT) screening of high-risk smokers reduces lung cancer (LC) specific mortality. Determining screening eligibility using individualised risk may improve screening effectiveness and reduce harm. Here, we compare the performance of two risk prediction models (PLCO and Liverpool Lung Project model (LLP)) and National Lung Screening Trial (NLST) eligibility criteria in a community-based screening programme.
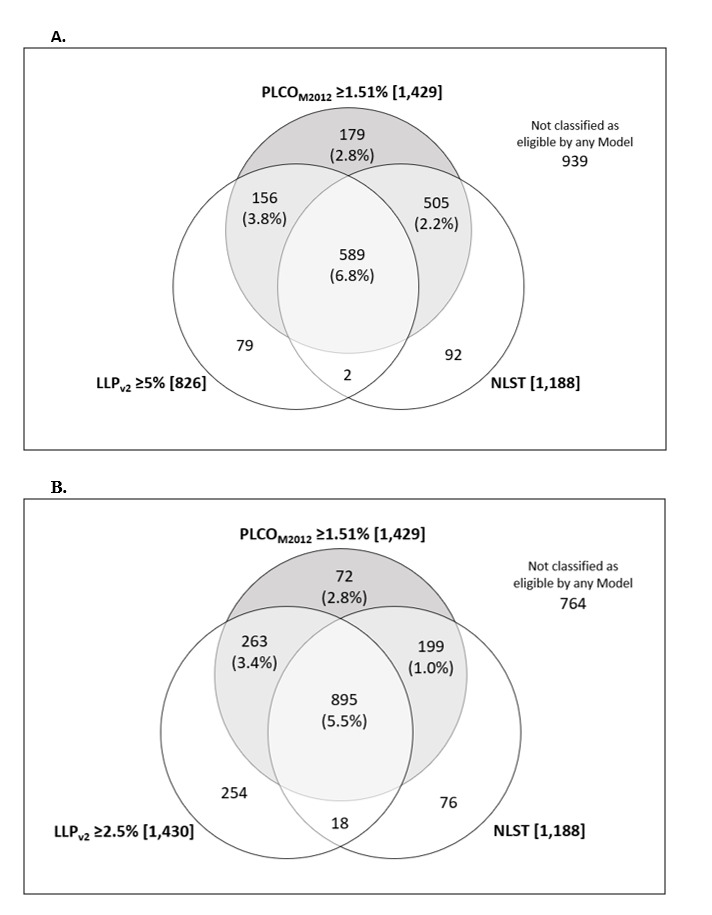
Ever-smokers aged 55-74, from deprived areas of Manchester, were invited to a Lung Health Check (LHC). Individuals at higher risk (PLCO score ≥1.51%) were offered annual LDCT screening over two rounds. LLP score was calculated but not used for screening selection; ≥2.5% and ≥5% thresholds were used for analysis.
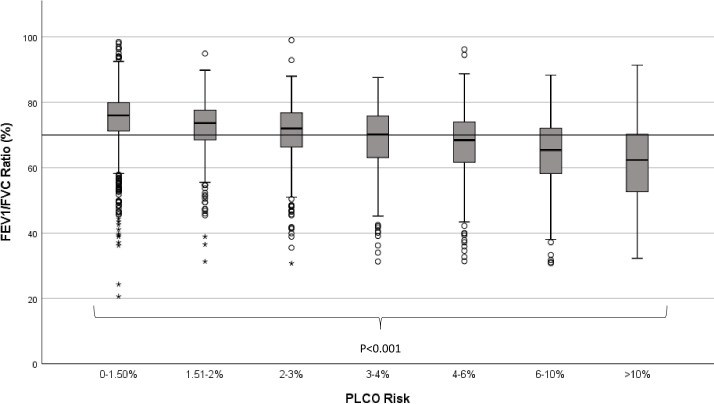
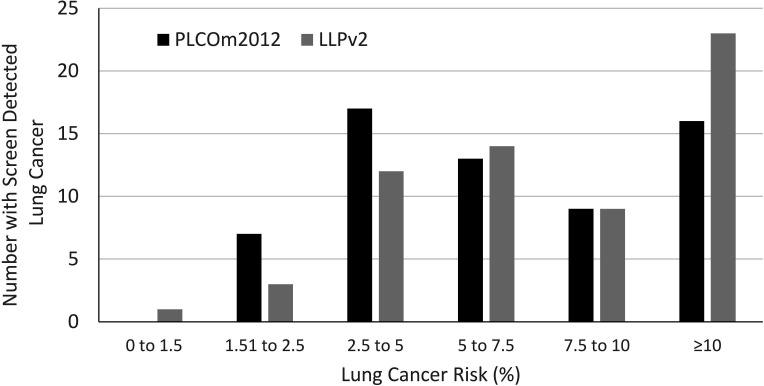
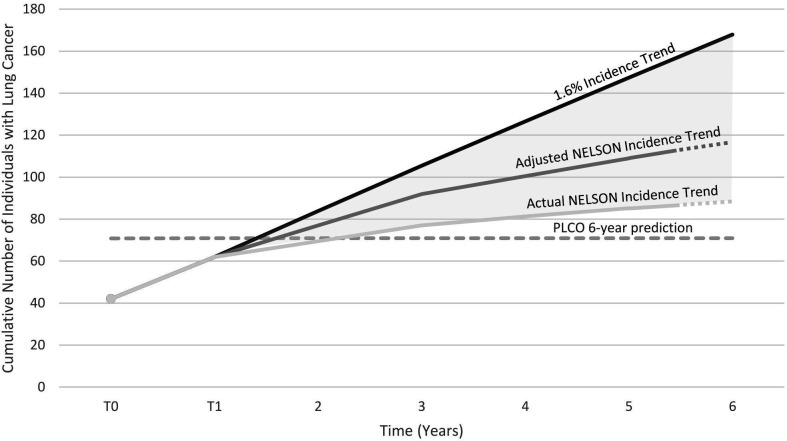
PLCO ≥1.51% selected 56% (n=1429) of LHC attendees for screening. LLP ≥2.5% also selected 56% (n=1430) whereas NLST (47%, n=1188) and LLP ≥5% (33%, n=826) selected fewer. Over two screening rounds 62 individuals were diagnosed with LC; representing 87% (n=62/71) of 6-year incidence predicted by mean PLCO score (5.0%). 26% (n=16/62) of individuals with LC were not eligible for screening using LLP ≥5%, 18% (n=11/62) with NLST criteria and 7% (n=5/62) with LLP ≥2.5%. NLST eligible Manchester attendees had 2.5 times the LC detection rate than NLST participants after two annual screens (≈4.3% (n=51/1188) vs 1.7% (n=438/26 309); p<0.0001). Adverse measures of health, including airflow obstruction, respiratory symptoms and cardiovascular disease, were positively correlated with LC risk. Coronary artery calcification was predictive of LC (OR 2.50, 95% CI 1.11 to 5.64; p=0.028).
Prospective comparisons of risk prediction tools are required to optimise screening selection in different settings. The PLCO model may underestimate risk in deprived UK populations; further research focused on model calibration is required.
低剂量 CT(LDCT)筛查高危吸烟者可降低肺癌(LC)特异性死亡率。使用个体化风险确定筛查资格可能会提高筛查效果并减少危害。在这里,我们比较了两种风险预测模型(PLCO 和利物浦肺项目模型(LLP))和国家肺癌筛查试验(NLST)在社区筛查计划中的表现。
邀请曼彻斯特贫困地区 55-74 岁的常吸烟者参加肺部健康检查(LHC)。风险较高的个体(PLCO 评分≥1.51%)接受两轮年度 LDCT 筛查。计算 LLP 评分,但不用于筛查选择;使用≥2.5%和≥5%的阈值进行分析。
PLCO≥1.51%选择了 LHC 参与者的 56%(n=1429)进行筛查。 LLP≥2.5%也选择了 56%(n=1430),而 NLST(47%,n=1188)和 LLP≥5%(33%,n=826)选择的人数较少。两轮筛查后,62 人被诊断患有 LC;占平均 PLCO 评分预测的 6 年发病率的 87%(n=62/71)(5.0%)。 LLP≥5%筛选不适用的 LC 患者占 26%(n=16/62),NLST 标准为 18%(n=11/62), LLP≥2.5%为 7%(n=5/62)。曼彻斯特 NLST 合格的参与者在两轮年度筛查后,LC 的检出率是 NLST 参与者的两倍半(≈4.3%(n=51/1188)vs 1.7%(n=438/26309);p<0.0001)。不良健康指标,包括气流阻塞、呼吸道症状和心血管疾病,与 LC 风险呈正相关。冠状动脉钙化是 LC 的预测因素(OR 2.50,95%CI 1.11-5.64;p=0.028)。
需要对风险预测工具进行前瞻性比较,以优化不同环境下的筛查选择。PLCO 模型可能低估了英国贫困人群的风险;需要进一步研究模型校准。