Guo Zhiyong, Xu Jinghong, Huang Shanzhou, Yin Meixian, Zhao Qiang, Ju Weiqiang, Wang Dongping, Gao Ningxin, Huang Changjun, Yang Lu, Chen Maogen, Zhang Zhiheng, Zhu Zebin, Wang Linhe, Zhu Caihui, Zhang Yixi, Tang Yunhua, Chen Haitian, Liu Kunpeng, Lu Yuting, Ma Yi, Hu Anbin, Chen Yinghua, Zhu Xiaofeng, He Xiaoshun
Organ Transplant Centre, The First Affiliated Hospital, Sun Yat-sen University, Guangzhou, China.
Guangdong Provincial Key Laboratory of Organ Donation and Transplant Immunology, Guangzhou, China.
Clin Transl Med. 2022 Apr;12(4):e546. doi: 10.1002/ctm2.546.
Ischemia-reperfusion injury (IRI) is considered an inherent component of organ transplantation that compromises transplant outcomes and organ availability. The ischemia-free liver transplantation (IFLT) procedure has been developed to avoid interruption of blood supply to liver grafts. It is unknown how IFLT might change the characteristics of graft IRI.
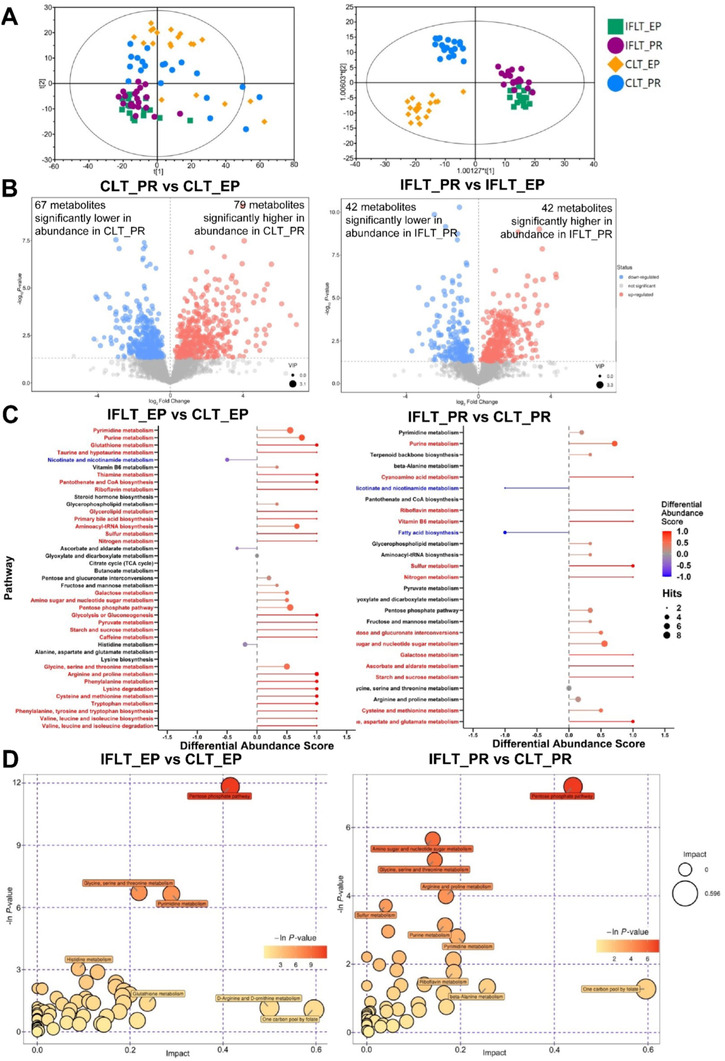
Serum and liver biopsy samples were collected from IFLT and conventional liver transplantation (CLT) recipients. Pathological, metabolomics, transcriptomics, and proteomics analyses were performed to identify the characteristic changes in graft IRI in IFLT.
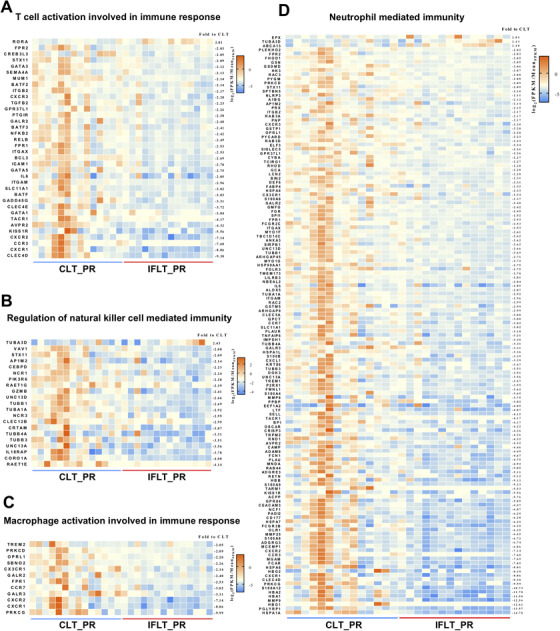
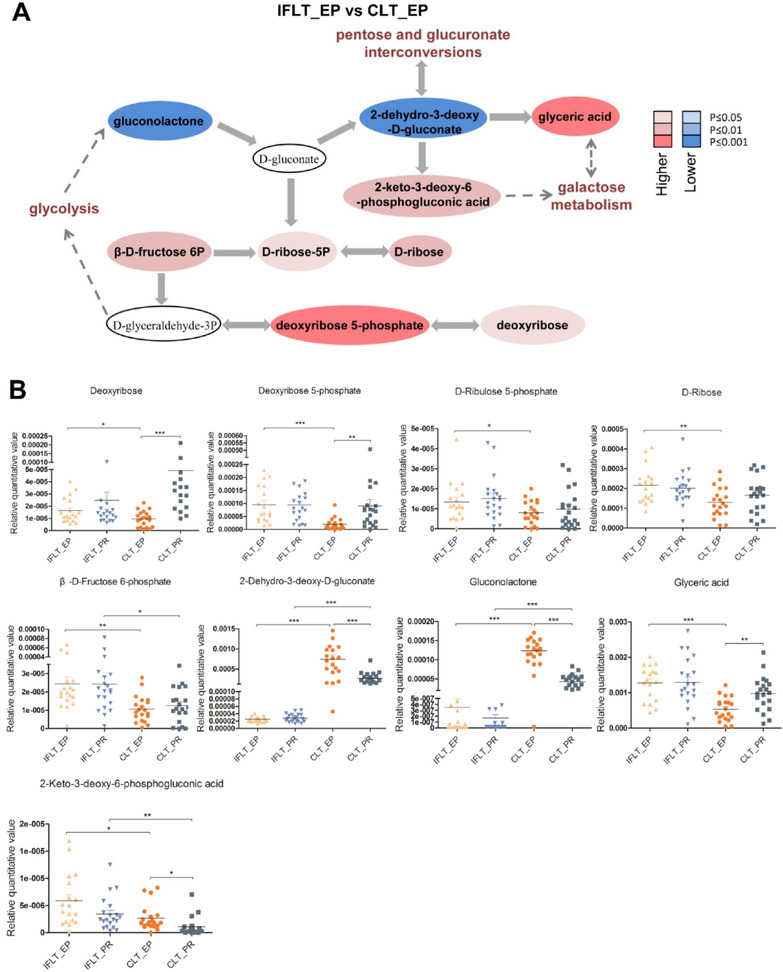
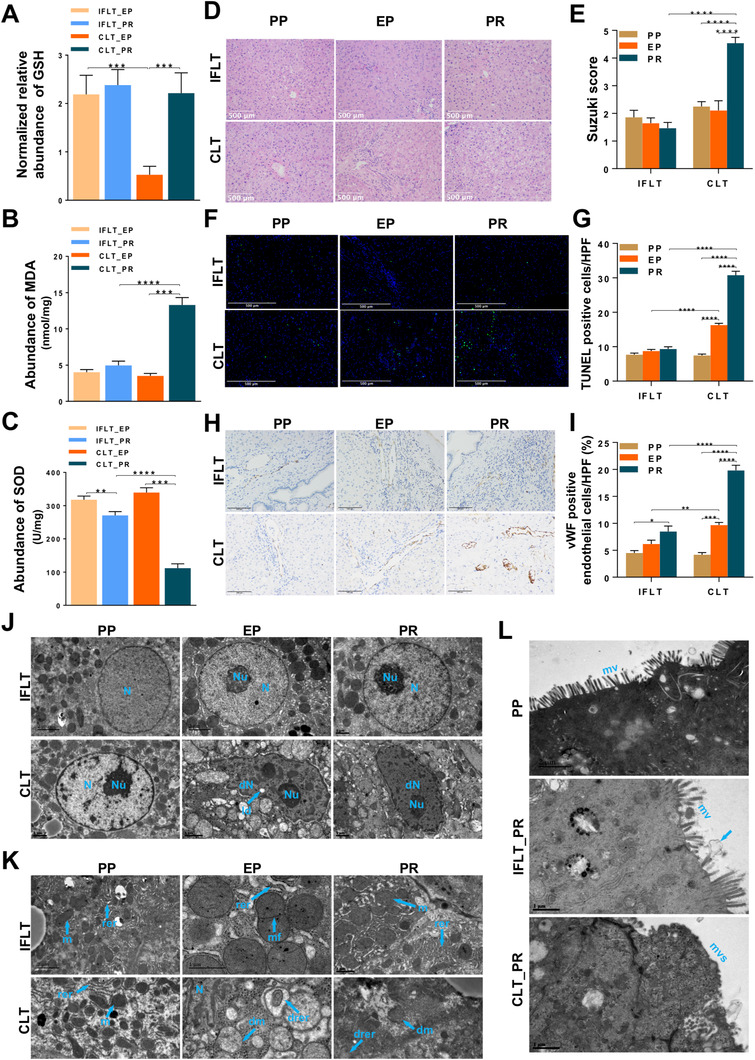
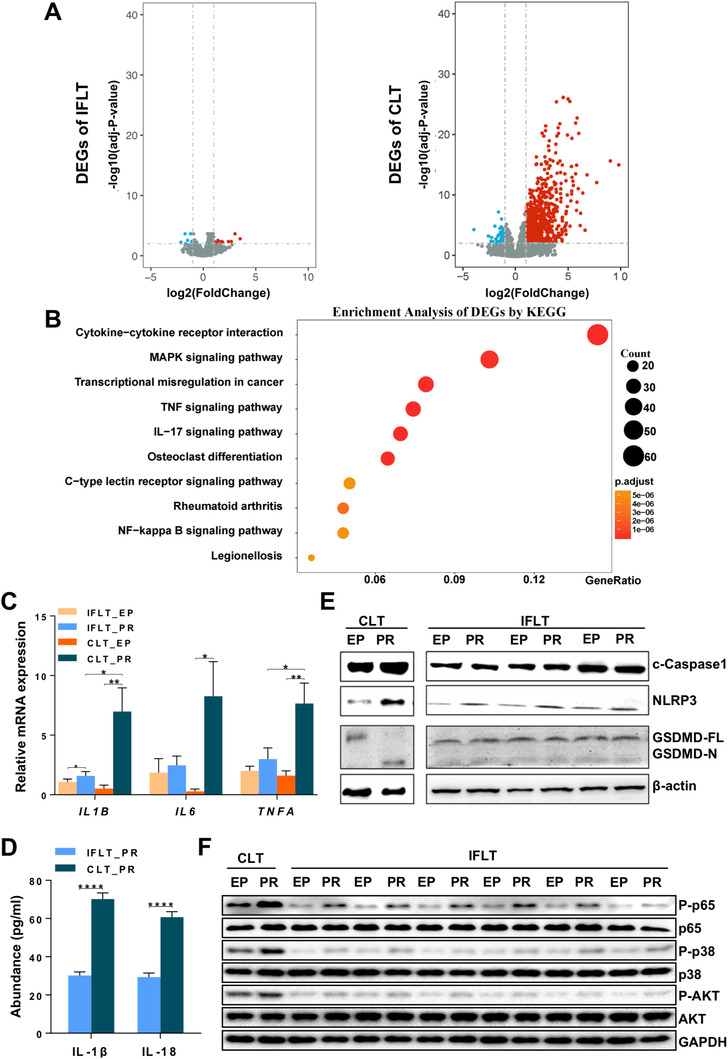
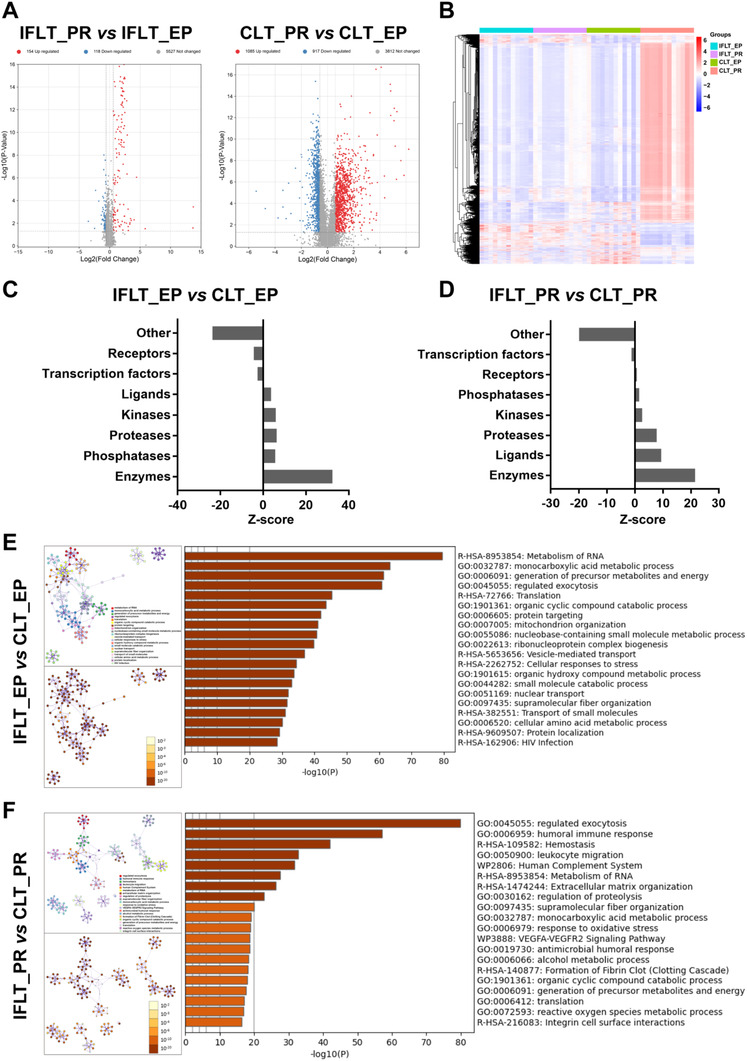
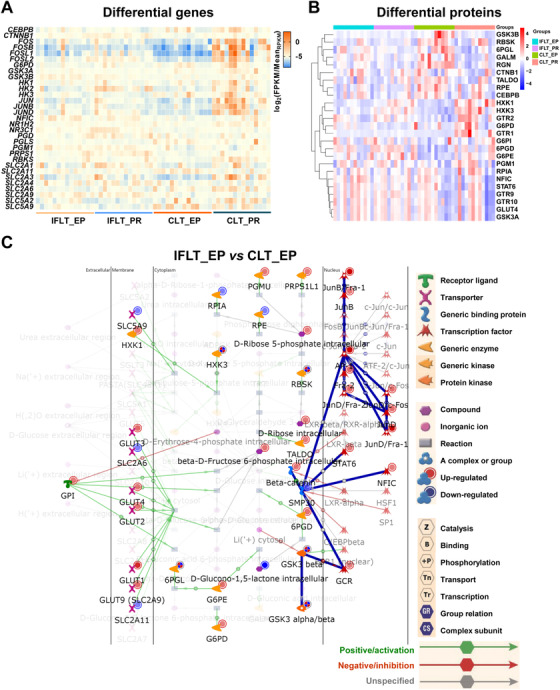
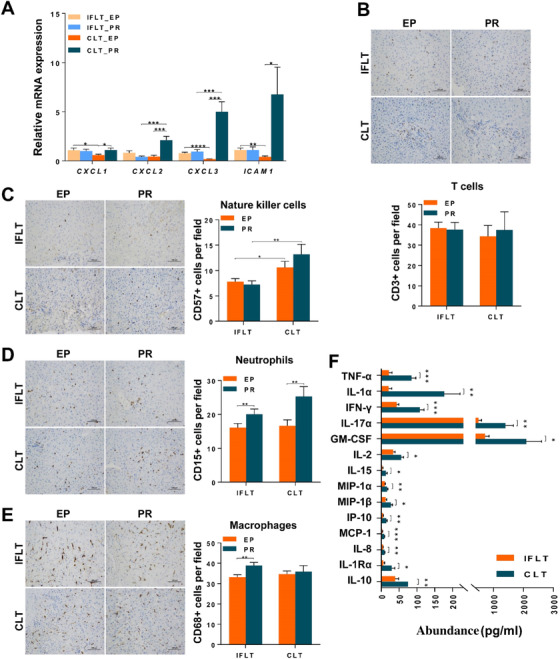
Peak aspartate aminotransferase (539.59 ± 661.76 U/L versus 2622.28 ± 3291.57 U/L) and alanine aminotransferase (297.64 ± 549.50 U/L versus 1184.16 ± 1502.76 U/L) levels within the first 7 days and total bilirubin levels by day 7 (3.27 ± 2.82 mg/dl versus 8.33 ± 8.76 mg/dl) were lower in the IFLT versus CLT group (all p values < 0.001). The pathological characteristics of IRI were more obvious in CLT grafts. The antioxidant pentose phosphate pathway remained active throughout the procedure in IFLT grafts and was suppressed during preservation and overactivated postrevascularization in CLT grafts. Gene transcriptional reprogramming was almost absent during IFLT but was profound during CLT. Proteomics analysis showed that "metabolism of RNA" was the major differentially expressed process between the two groups. Several proinflammatory pathways were not activated post-IFLT as they were post-CLT. The activities of natural killer cells, macrophages, and neutrophils were lower in IFLT grafts than in CLT grafts. The serum levels of 14 cytokines were increased in CLT versus IFLT recipients.
IFLT can largely avoid the biological consequences of graft IRI, thus has the potential to improve transplant outcome while increasing organ utilization.
缺血再灌注损伤(IRI)被认为是器官移植的一个固有组成部分,它会影响移植结果和器官的可获得性。无缺血肝移植(IFLT)手术旨在避免肝移植物血液供应的中断。目前尚不清楚IFLT如何改变移植物IRI的特征。
收集IFLT和传统肝移植(CLT)受者的血清和肝活检样本。进行病理、代谢组学、转录组学和蛋白质组学分析,以确定IFLT中移植物IRI的特征性变化。
IFLT组在术后第1周内的天冬氨酸转氨酶峰值(539.59±661.76 U/L 对比2622.28±3291.57 U/L)和丙氨酸转氨酶峰值(297.64±549.50 U/L对比1184.16±1502.76 U/L)以及第7天的总胆红素水平(3.27±2.82 mg/dl对比8.33±8.76 mg/dl)均低于CLT组(所有p值<0.001)。CLT移植物中IRI的病理特征更为明显。抗氧化戊糖磷酸途径在IFLT移植物的整个过程中保持活跃,而在CLT移植物的保存过程中受到抑制,再灌注后过度激活。在IFLT过程中几乎没有基因转录重编程,但在CLT过程中则很显著。蛋白质组学分析表明,“RNA代谢”是两组之间主要的差异表达过程。与CLT后不同,IFLT后几种促炎途径未被激活。IFLT移植物中自然杀伤细胞、巨噬细胞和中性粒细胞的活性低于CLT移植物。CLT受者血清中14种细胞因子的水平高于IFLT受者。
IFLT可以很大程度上避免移植物IRI的生物学后果,因此有可能改善移植结果并提高器官利用率。