Department of Urology, Kyushu University, Fukuoka, Japan.
Department of Urology, The Jikei University School of Medicine, Tokyo, Japan.
Cancer Sci. 2022 Jul;113(7):2386-2396. doi: 10.1111/cas.15383. Epub 2022 May 17.
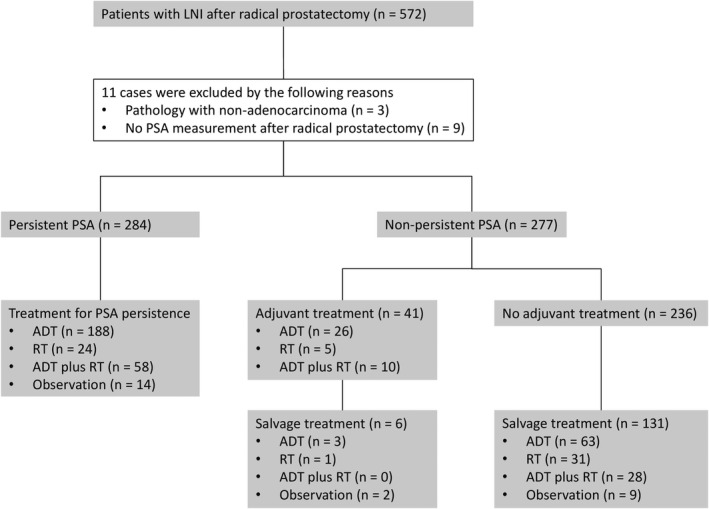
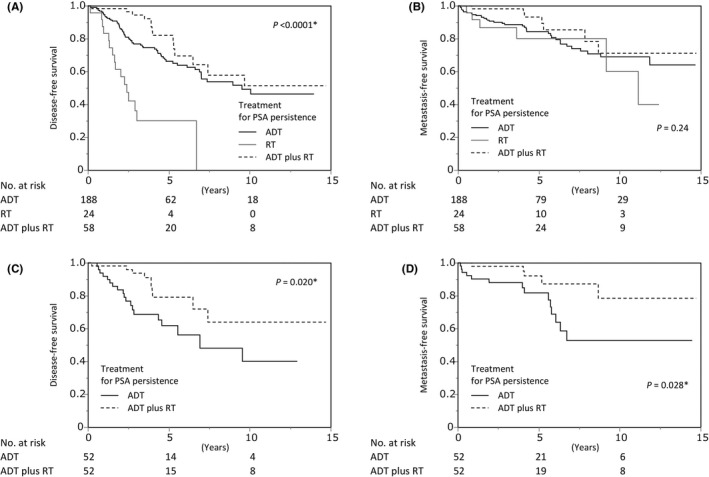
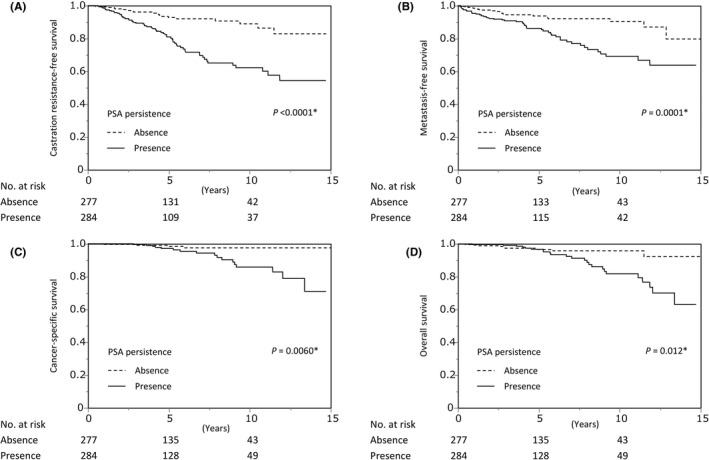
The treatment for lymph node involvement (LNI) after radical prostatectomy (RP) has not been established. This study aimed to reveal the outcomes of various management strategies among patients with LNI after RP. Retrospectively, 561 patients with LNI after pelvic lymph node dissection (PLND) with RP treated between 2006 and 2019 at 33 institutions participating in the Japanese Urological Oncology Group were investigated. Metastasis-free survival (MFS) was the primary outcome. Patients were stratified by prostate-specific antigen (PSA) persistence after RP. Cox regression models were used to analyze the relationships between clinicopathological characteristics and survival. Survival analyses were conducted using the Kaplan-Meier method and log-rank test with or without propensity score matching. Prognoses, including MFS and overall survival, were prominently inferior among patients with persistent PSA compared with those without persistent PSA. In multivariate analysis, androgen deprivation therapy (ADT) plus radiotherapy (RT) was associated with better MFS than ADT alone among patients with persistent PSA (hazard ratio = 0.37; 95% confidence interval = 0.15-0.93; p = 0.034). Similarly, MFS and overall survival were significantly better for ADT plus RT than for ADT alone among patients with persistent PSA after propensity score matching. This study indicated that PSA persistence in LNI prostate cancer increased the risk of poor prognoses, and intensive treatment featuring the addition of RT to ADT might improve survival.
根治性前列腺切除术后(RP)淋巴结受累(LNI)的治疗尚未确定。本研究旨在揭示 RP 后 LNI 患者的各种管理策略的结果。回顾性分析了 2006 年至 2019 年期间在参与日本泌尿肿瘤学组的 33 个机构接受盆腔淋巴结清扫术(PLND)联合 RP 治疗的 561 例 LNI 患者的资料。无转移生存(MFS)是主要结局。根据 RP 后前列腺特异性抗原(PSA)的持续情况对患者进行分层。使用 Cox 回归模型分析临床病理特征与生存之间的关系。使用 Kaplan-Meier 方法和对数秩检验进行生存分析,无论是否进行倾向评分匹配。与无 PSA 持续患者相比,PSA 持续患者的预后,包括 MFS 和总生存,明显较差。多变量分析显示,与 ADT 单药治疗相比,PSA 持续患者中 ADT 联合放疗(RT)与更好的 MFS 相关(风险比=0.37;95%置信区间=0.15-0.93;p=0.034)。同样,在倾向评分匹配后,PSA 持续患者中 ADT 联合 RT 的 MFS 和总生存均明显优于 ADT 单药治疗。本研究表明,LNI 前列腺癌中 PSA 的持续存在增加了预后不良的风险,并且将 RT 加入 ADT 的强化治疗可能会改善生存。