Molano Alejandra P, Hutchison Colin A, Sanchez Ricardo, Rivera Angela S, Buitrago Giancarlo, Dazzarola María P, Munevar Mario, Guerrero Mauricio, Vesga Jasmín I, Sanabria Mauricio
Baxter Renal Care Services-Agencia Cardioinfantil, Bogotá, DC, Colombia.
Department of Medicine, Hawke's Bay District Health Board, Hastings, New Zealand.
Kidney Med. 2022 Feb 7;4(4):100431. doi: 10.1016/j.xkme.2022.100431. eCollection 2022 Apr.
RATIONALE & OBJECTIVE: This study investigated the effects on patients' outcomes of using medium cutoff (MCO) versus high-flux (HF) dialysis membranes.
A retrospective, observational, multicenter, cohort study.
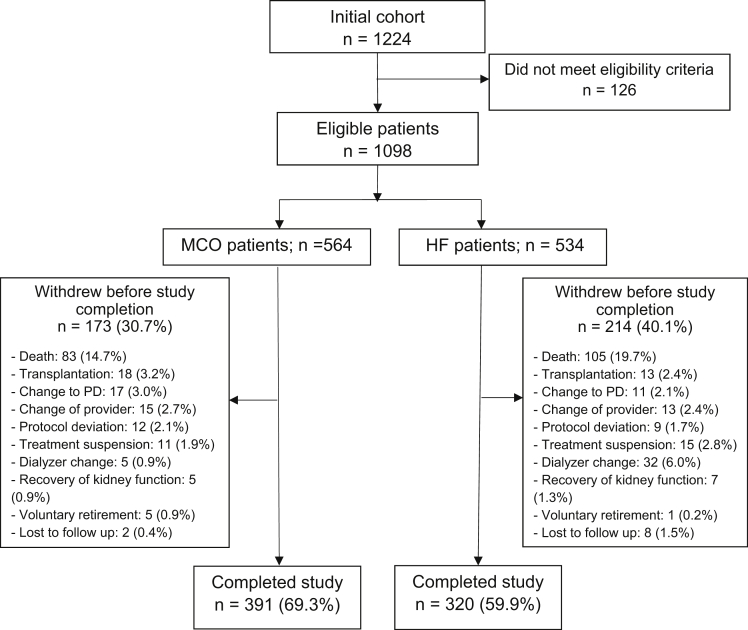
SETTING & PARTICIPANTS: Patients aged greater than 18 years receiving hemodialysis at the Baxter Renal Care Services dialysis network in Colombia. The inception of the cohort occurred from September 1, 2017, to November 30, 2017, with follow-up to November 30, 2019.
The patients were divided into 2 cohorts according to the dialyzer used at the inception: (1) MCO membrane or (2) HF membrane.
Primary outcomes were the hospitalization rate from any cause and hospitalization days per patient-year. Secondary outcomes were acute cardiovascular events and mortality rates from any cause and secondary to cardiovascular causes. Laboratory parameters were assessed throughout the 2-year follow-up period.
Descriptive statistics were used to report population characteristics. Inverse probability of treatment weighting was applied to each group before analysis. All categorical variables were compared using Pearson's χ test, and continuous variables were analyzed with the test. Baseline differences between groups with a value of >10% were considered clinically meaningful. Laboratory variables were measured at 5 consecutive time points. A between-patient effect was analyzed using a split-plot factorial analysis of variance.
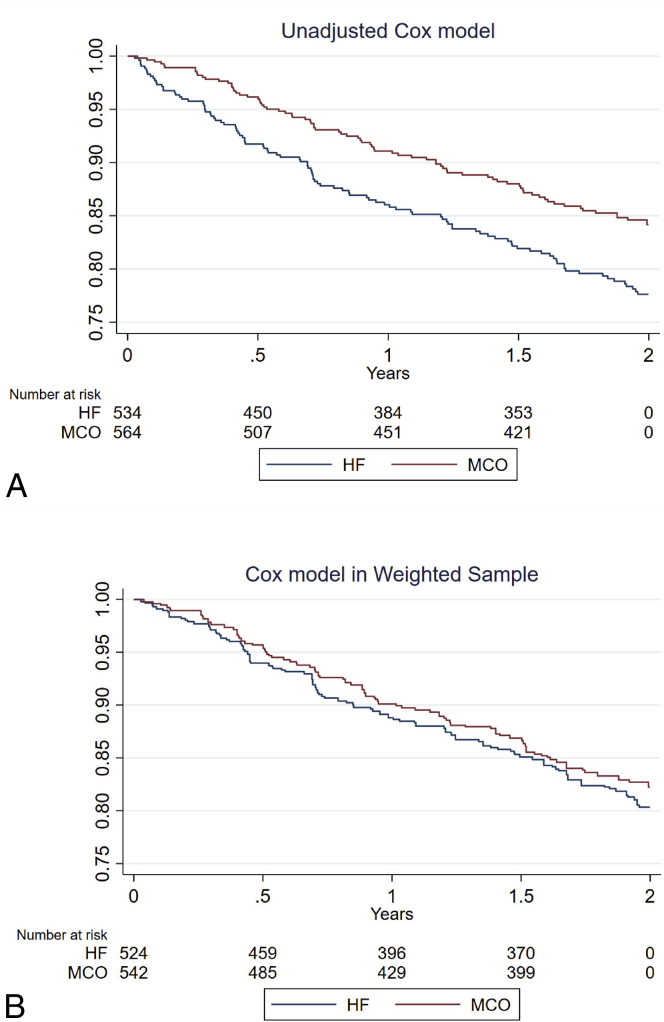
The analysis included 1,098 patients, of whom 564 (51.3%) were dialyzed with MCO membranes and 534 (48.7%) with HF membranes. Patients receiving hemodialysis with MCO membranes had a lower all-cause hospitalization incidence rate (IR) per patient-year (IR = 0.93; 95% CI, 0.82-1.03) than those receiving hemodialysis with HF membranes (IR = 1.13; 95% CI, 0.96-1.30), corresponding to a significant incident rate ratio (MCO/HF) of 0.82 (95% CI, 0.68-0.99; = 0.04). The frequency of nonfatal cardiovascular events showed statistical significance, with a lower incidence in the MCO group (incident rate ratio = 0.66; 95% CI, 0.46-0.96; = 0.03). No statistically significant differences in all-cause time until death were observed ( = 0.48). Albumin levels were similar between the 2 dialyzer cohorts.
Despite the robust statistical analysis, there remains the possibility that unmeasured variables may still generate residual imbalance and, therefore, skew the results.
The incidences of hospitalization and cardiovascular events in patients receiving hemodialysis were lower when dialyzed with MCO membranes than HF membranes. A randomized controlled trial would be desirable to confirm these results.
Clinical Trials.gov, ISRCTN12403265.
本研究调查了使用中通量(MCO)与高通量(HF)透析膜对患者预后的影响。
一项回顾性、观察性、多中心队列研究。
年龄大于18岁、在哥伦比亚百特肾脏护理服务透析网络接受血液透析的患者。队列起始时间为2017年9月1日至2017年11月30日,随访至2019年11月30日。
根据起始时使用的透析器将患者分为2个队列:(1)MCO膜组或(2)HF膜组。
主要结局指标为任何原因导致的住院率及每位患者每年的住院天数。次要结局指标为急性心血管事件、任何原因及心血管原因导致的死亡率。在整个2年随访期内评估实验室参数。
采用描述性统计报告人群特征。在分析前对每组应用治疗权重的逆概率。所有分类变量采用Pearson卡方检验进行比较,连续变量采用t检验进行分析。组间基线差异>10%被认为具有临床意义。实验室变量在连续5个时间点进行测量。采用裂区析因方差分析分析患者间效应。
分析纳入1098例患者,其中564例(51.3%)使用MCO膜进行血液透析,534例(48.7%)使用HF膜进行血液透析。使用MCO膜进行血液透析的患者每位患者每年的全因住院发病率(IR)(IR = 0.93;95%CI,0.82 - 1.03)低于使用HF膜进行血液透析的患者(IR = 1.13;95%CI,0.96 - 1.30),相应的全因发病率比(MCO/HF)为0.82(95%CI,0.68 - 0.99;P = 0.04)。非致命心血管事件的发生率具有统计学意义,MCO组发生率较低(发病率比 = 0.66;95%CI,0.46 - 0.96;P = 0.03)。在全因死亡时间方面未观察到统计学显著差异(P = 0.48)。两个透析器队列之间的白蛋白水平相似。
尽管进行了强有力的统计分析,但仍有可能存在未测量的变量导致残留不平衡,从而使结果产生偏差。
使用MCO膜进行血液透析的患者的住院率和心血管事件发生率低于使用HF膜进行血液透析的患者。需要进行一项随机对照试验来证实这些结果。
ClinicalTrials.gov,ISRCTN12403265。