Zelnick Leila R, Shlipak Michael G, Soliman Elsayed Z, Anderson Amanda, Christenson Robert, Kansal Mayank, Deo Rajat, He Jiang, Jaar Bernard G, Weir Matthew R, Rao Panduranga, Cohen Debbie L, Cohen Jordana B, Feldman Harold I, Go Alan, Bansal Nisha
Kidney Research Institute, Department of Medicine (Nephrology), University of Washington, Seattle, Washington, USA.
Department of Medicine, University of California San Francisco, San Francisco, California, USA.
Kidney Int Rep. 2022 Feb 2;7(4):708-719. doi: 10.1016/j.ekir.2022.01.1067. eCollection 2022 Apr.
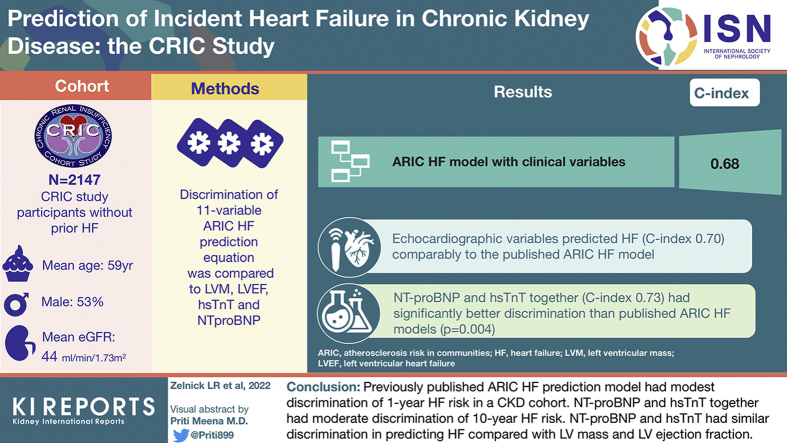
Heart failure (HF) is common in chronic kidney disease (CKD); identifying patients with CKD at high risk for HF may guide clinical care. We assessed the prognostic value of cardiac biomarkers and echocardiographic variables for 10-year HF prediction compared with a published clinical HF prediction equation in a cohort of participants with CKD.
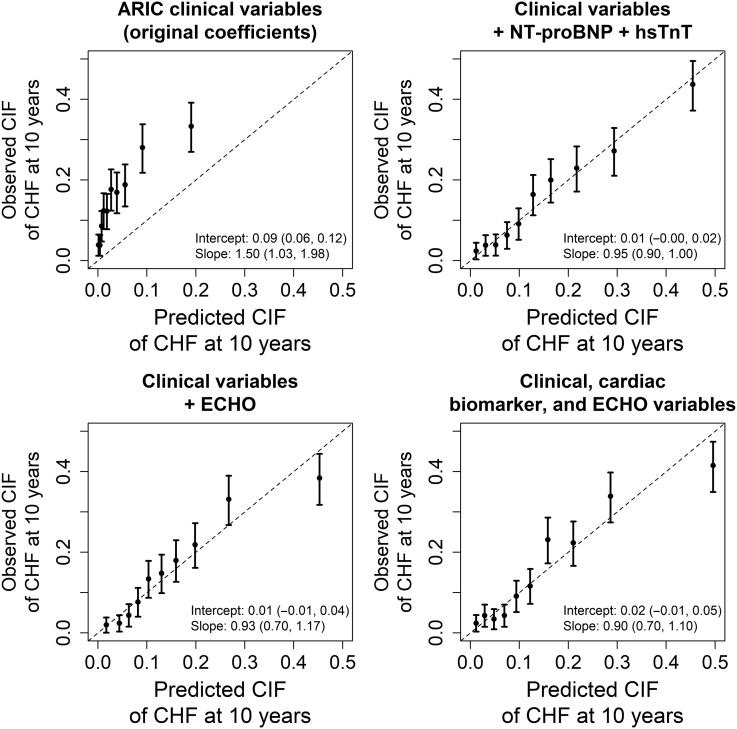
We studied 2147 Chronic Renal Insufficiency Cohort (CRIC) participants without prior HF with complete clinical, cardiac biomarker (N-terminal brain natriuretic peptide [NT-proBNP] and high sensitivity troponin-T [hsTnT]), and echocardiographic data (left ventricular mass [LVM] and left ventricular ejection fraction [LVEF] data). We compared the discrimination of the 11-variable Atherosclerosis Risk in Communities (ARIC) HF prediction equation with LVM, LVEF, hsTnT, and NT-proBNP to predict 10-year risk of hospitalization for HF using a Fine and Gray modeling approach. We separately evaluated prediction of HF with preserved and reduced LVEF (LVEF ≥50% and <50%, respectively). We assessed discrimination with internally valid C-indices using 10-fold cross-validation.
Participants' mean (SD) age was 59 (11) years, 53% were men, 43% were Black, and mean (SD) estimated glomerular filtration rate (eGFR) was 44 (16) ml/min per 1.73 m. A total of 324 incident HF hospitalizations occurred during median (interquartile range) 10.0 (5.7-10.0) years of follow-up. The ARIC HF model with clinical variables had a C-index of 0.68. Echocardiographic variables predicted HF (C-index 0.70) comparably to the published ARIC HF model, while NT-proBNP and hsTnT together (C-index 0.73) had significantly better discrimination ( = 0.004). A model including cardiac biomarkers, echocardiographic variables, and clinical variables had a C-index of 0.77. Discrimination of HF with preserved LVEF was lower than for HF with reduced LVEF for most models.
The ARIC HF prediction model for 10-year HF risk had modest discrimination among adults with CKD. NT-proBNP and hsTnT discriminated better than the ARIC HF model and at least as well as a model with echocardiographic variables. HF clinical prediction models tailored to adults with CKD are needed. Until then, measurement of NT-proBNP and hsTnT may be a low-burden approach to predicting HF in this population, as they offer moderate discrimination.
心力衰竭(HF)在慢性肾脏病(CKD)中很常见;识别CKD中发生HF高风险的患者可能会指导临床护理。我们评估了心脏生物标志物和超声心动图变量对10年HF预测的预后价值,并与已发表的临床HF预测方程在一组CKD参与者中进行比较。
我们研究了2147名慢性肾功能不全队列(CRIC)参与者,他们既往无HF,有完整的临床、心脏生物标志物(N末端脑钠肽前体[NT-proBNP]和高敏肌钙蛋白T[hsTnT])以及超声心动图数据(左心室质量[LVM]和左心室射血分数[LVEF]数据)。我们使用Fine和Gray建模方法,比较了包含11个变量的社区动脉粥样硬化风险(ARIC)HF预测方程与LVM、LVEF、hsTnT和NT-proBNP对10年HF住院风险的预测能力。我们分别评估了LVEF保留和降低(分别为LVEF≥50%和<50%)时HF的预测情况。我们使用10倍交叉验证,通过内部有效C指数评估区分度。
参与者的平均(标准差)年龄为59(11)岁,53%为男性,43%为黑人,平均(标准差)估计肾小球滤过率(eGFR)为44(16)ml/min/1.73m²。在中位(四分位间距)10.0(5.7 - 10.0)年的随访期间,共发生324例HF住院事件。包含临床变量的ARIC HF模型的C指数为0.68。超声心动图变量对HF的预测能力(C指数0.70)与已发表的ARIC HF模型相当,而NT-proBNP和hsTnT联合使用时(C指数0.73)具有显著更好的区分度(P = 0.004)。一个包含心脏生物标志物、超声心动图变量和临床变量的模型的C指数为0.77。对于大多数模型,LVEF保留的HF的区分度低于LVEF降低的HF。
用于预测10年HF风险的ARIC HF预测模型在患有CKD的成年人中区分度一般。NT-proBNP和hsTnT的区分度优于ARIC HF模型,且至少与包含超声心动图变量的模型相当。需要为患有CKD的成年人量身定制HF临床预测模型。在此之前,测量NT-proBNP和hsTnT可能是预测该人群HF的一种低负担方法,因为它们具有中等区分度。