London School of Economics and Political Science.
Program on Regulation, Therapeutics, and Law (PORTAL), Brigham and Women's Hospital and Harvard Medical School.
Milbank Q. 2022 Jun;100(2):562-588. doi: 10.1111/1468-0009.12565. Epub 2022 May 3.
Policy Points Only a small minority of new drugs in "nonprotected" classes are widely covered by Part D plans nationwide in the year after US Food and Drug Administration (FDA) approval. Part D plans frequently apply utilization management restrictions such as prior authorizations to newly approved drugs in both protected and nonprotected classes. Drug price influences both formulary inclusion (in nonprotected classes) and coverage restrictions (in both protected and nonprotected classes), while other drug characteristics such as therapeutic benefits are not consistently associated with formulary design. Plans do not seem to favor the minority of drugs that are determined to offer added therapeutic benefit over existing alternatives.
Medicare Part D is an outpatient prescription drug benefit for older Americans covering more than 46 million beneficiaries. Except for mandatory coverage for essentially all drugs in six protected classes, plans have substantial flexibility in how they design their formularies: which drugs are covered, which drugs are subject to restrictions, and what factors determine formulary placement. Our objective in this paper was to document the extent to which Part D plans limit coverage of newly approved drugs.
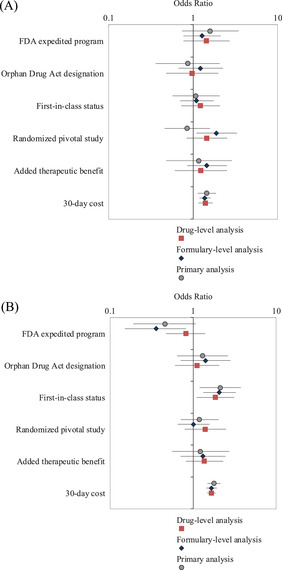
We examined the formulary design of 4,582 Part D plans from 2014 through 2018 and measured (1) the decision to cover newly approved drugs in nonprotected classes, (2) use of utilization management tools in protected and nonprotected classes, and (3) the association between plan design and drug-level characteristics such as 30-day cost, therapeutic benefit, and the US Food and Drug Administration (FDA) expedited regulatory pathway.
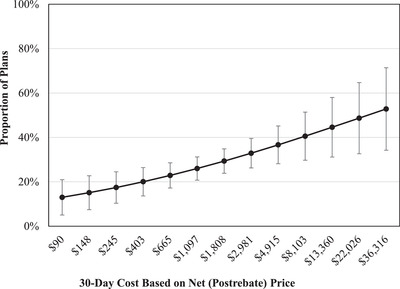
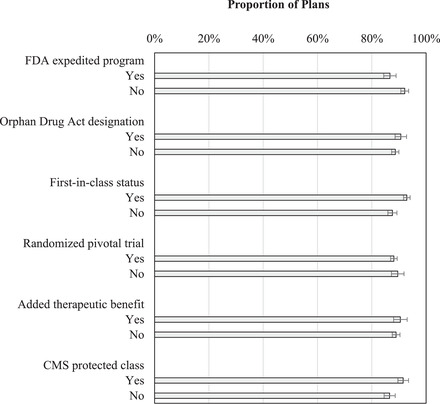
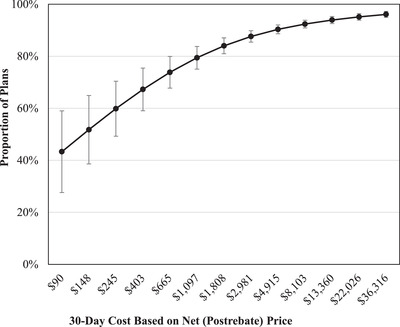
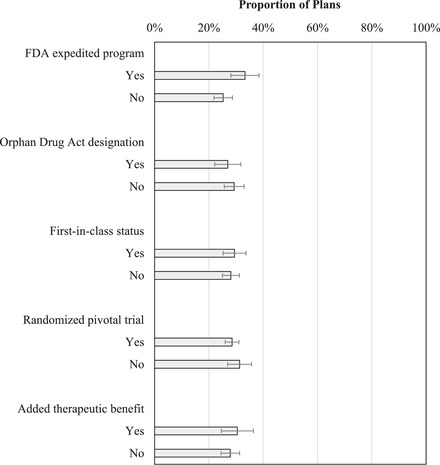
The FDA approved 109 new drugs predominantly used in outpatient settings between 2013 and 2017. Of these, 75 fell outside of the six protected drug classes. One-fifth of drugs in nonprotected classes (15 out of 75) were covered by more than half of plans during the first year after approval. Coverage was often conditional on utilization management strategies in both protected and nonprotected classes: only seven drugs (6%) were covered without prior authorization requirements in more than half of plans. Higher 30-day drug costs were associated with more widespread coverage in nonprotected classes: drugs that cost less than $150 for a 30-day course were covered by fewer than 20% of plans while those that cost more than $30,000 per 30 days were covered by more than 50% of plans. Plans were also more likely to implement utilization management tools on high-cost drugs in both protected and nonprotected classes. A higher proportion of plans implemented utilization management strategies on covered drugs with first-in-class status than drugs that were not first in class. Other drug characteristics, including availability of added therapeutic benefit and inclusion in FDA expedited regulatory approval, were not consistently associated with plan coverage or formulary restrictions.
Newly approved drugs are frequently subject to formulary exclusions and restrictions in Medicare Part D. Ensuring that formulary design in Part D is linked closely to the therapeutic value of newly approved drugs would improve patients' welfare.
本研究旨在记录医疗保险 Part D 计划限制新批准药物覆盖范围的程度。
我们研究了 2014 年至 2018 年的 4582 个医疗保险 Part D 计划的处方设计,衡量了(1)非保护类新药的覆盖决策,(2)保护类和非保护类新药的利用管理工具使用情况,以及(3)计划设计与药物水平特征(如 30 天费用、治疗效益和美国食品和药物管理局(FDA)加速监管途径)之间的关联。
FDA 在 2013 年至 2017 年期间批准了 109 种主要用于门诊的新药。其中,75 种药物不属于六个受保护的药物类别。在批准后的第一年,非保护类药物中有五分之一(75 种中的 15 种)被超过一半的计划所覆盖。覆盖范围通常取决于保护类和非保护类药物中的利用管理策略:只有七种药物(6%)在超过一半的计划中无需事先授权要求即可覆盖。较高的 30 天药物成本与非保护类药物更广泛的覆盖范围相关:30 天疗程费用低于 150 美元的药物,仅有不到 20%的计划覆盖,而 30 天费用超过 30000 美元的药物,超过 50%的计划覆盖。保护类和非保护类药物中,计划更有可能对高成本药物实施利用管理工具。在覆盖药物中,具有同类首创地位的药物比非同类首创药物更有可能实施利用管理策略。其他药物特征,包括附加治疗效益的可用性和纳入 FDA 加速监管批准,与计划覆盖或处方限制没有一致的关联。
医疗保险 Part D 中的新批准药物经常受到处方排除和限制。确保 Part D 中的处方设计与新批准药物的治疗价值密切相关,将提高患者的福利。