Department of Family and Community Medicine, University of Toronto, Toronto, ON, Canada.
Department of Medicine, Division of Endocrinology, University of British Columbia, Vancouver, BC, Canada.
Arch Osteoporos. 2022 May 6;17(1):75. doi: 10.1007/s11657-022-01110-z.
In many countries, osteoporosis is predominantly managed by primary care physicians; however, management after a fragility fracture has not been widely investigated. We describe osteoporosis care gaps in a real-world patient cohort. Our findings help inform initiatives to identify and overcome obstacles to effective management of patients after fragility fracture.
A fragility fracture is a major risk factor for subsequent fracture in adults aged ≥ 50 years. This retrospective observational study aimed to characterize post-fracture management in Canadian primary care.
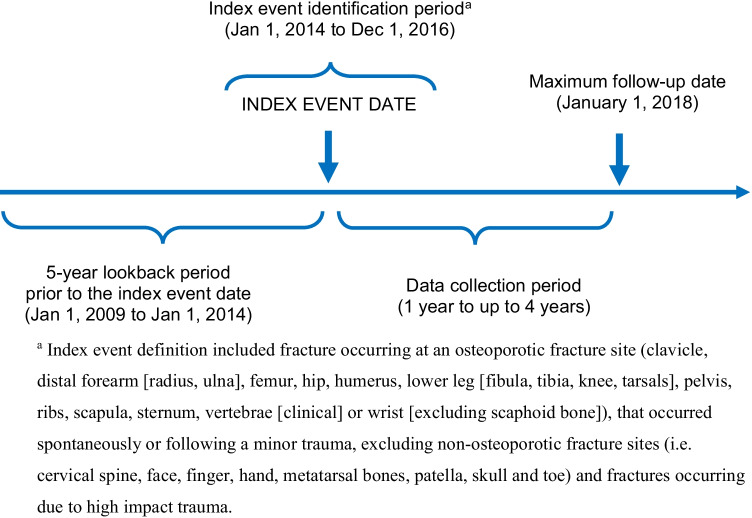
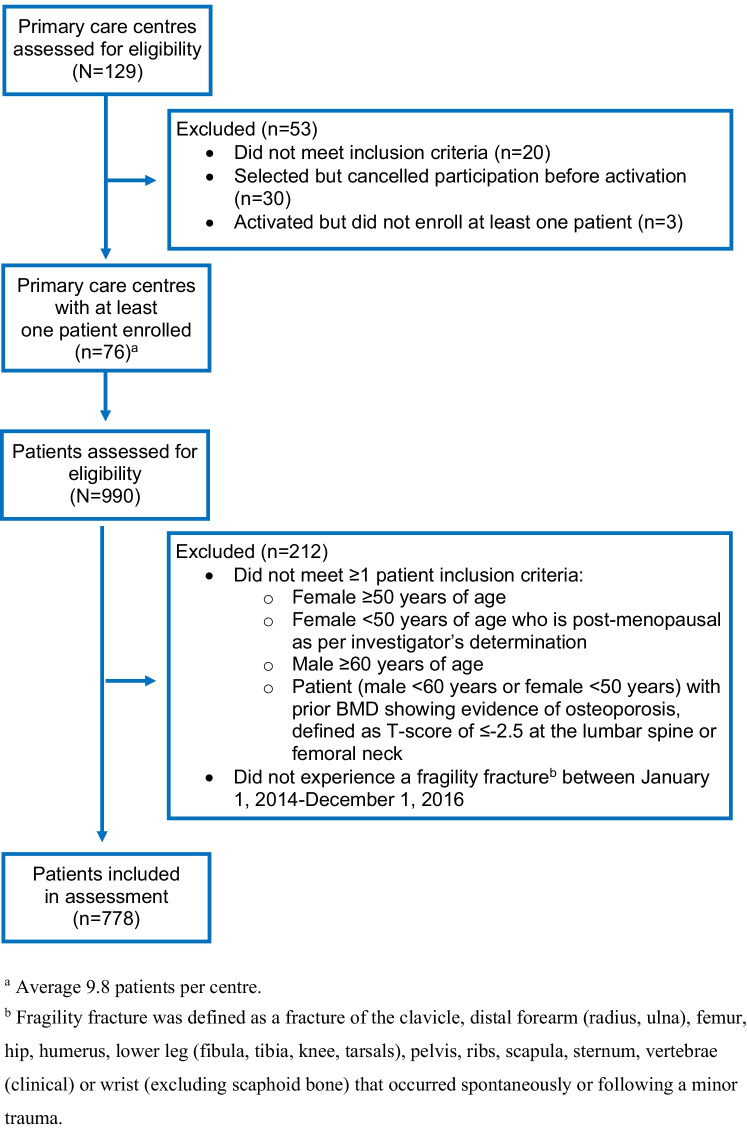
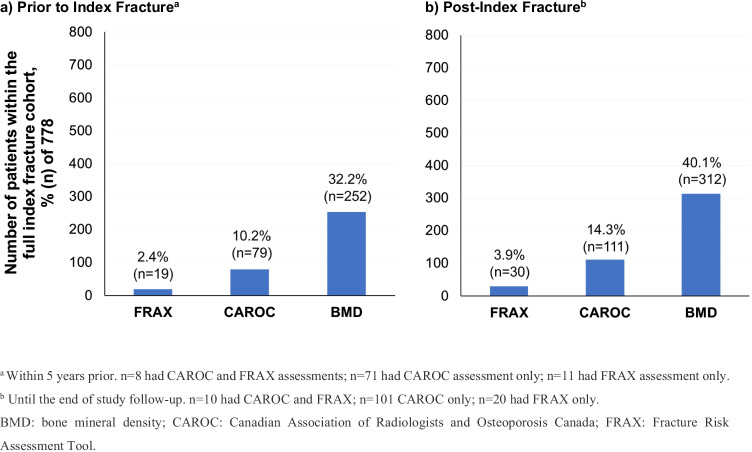
A total of 778 patients with an index fragility fracture (low-trauma, excluding small bones) occurring between 2014 and 2016 were identified from medical records at 76 primary care centers in Canada, with follow-up until January 2018.
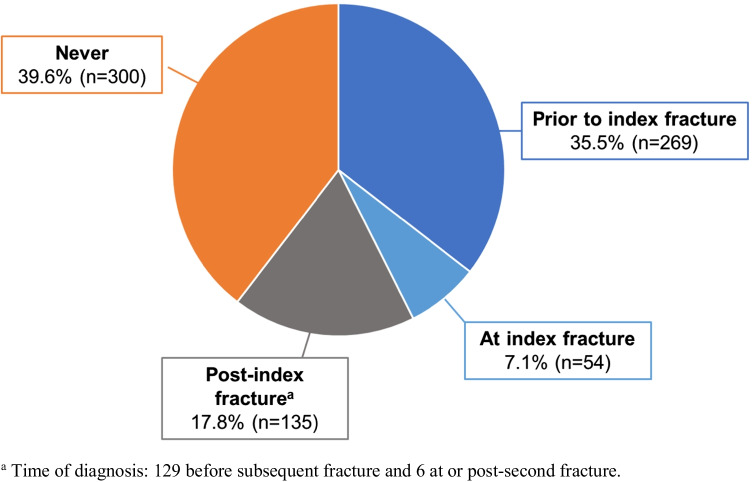
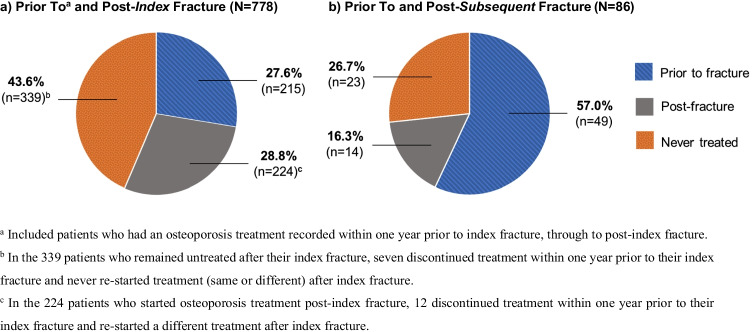
Of 778 patients (80.5% female, median age [IQR] 73 [64-80]), 215 were on osteoporosis treatment and 269 had osteoporosis diagnosis recorded prior to their index fracture. The median follow-up was 363 (IQR 91-808) days. Of patients not on osteoporosis treatment at their index fracture, 60.2% (n = 339/563) remained untreated after their index fracture and 62.2% (n = 23/37) continued untreated after their subsequent fracture. After their index fracture, fracture risk assessment (FRAX or CAROC) was not performed in 83.2% (n = 647/778) of patients, and 59.9% (n = 466/778) of patients did not receive bone mineral density testing. Of patients without osteoporosis diagnosis recorded prior to their index date, 61.3% (n = 300/489) remained undiagnosed after their index fracture. At least one subsequent fracture occurred in 11.5% (n = 86/778) of patients.
In the primary care setting, fragility fracture infrequently resulted in osteoporosis treatment or fracture risk assessment, even after multiple fragility fractures. These results suggest a fragility fracture is not recognized as a major risk factor for subsequent fracture and its occurrence does not prompt primary care physicians to intervene. These data urge initiatives to identify and overcome obstacles to primary care physicians' effective management of patients after fragility fractures.
在许多国家,骨质疏松症主要由初级保健医生管理;然而,脆性骨折后的管理尚未得到广泛研究。我们描述了真实患者队列中骨质疏松症护理的差距。我们的研究结果有助于为识别和克服脆性骨折后患者有效管理的障碍提供信息。
脆性骨折是 50 岁及以上成年人再次骨折的主要危险因素。这项回顾性观察性研究旨在描述加拿大初级保健中的骨折后管理情况。
从加拿大 76 个初级保健中心的病历中确定了 778 例(2014 年至 2016 年)索引脆性骨折(低创伤,不包括小骨头)患者,随访至 2018 年 1 月。
778 例患者中(80.5%为女性,中位数年龄[IQR]73[64-80]),215 例接受骨质疏松症治疗,269 例在指数骨折前有骨质疏松症诊断记录。中位随访时间为 363(IQR 91-808)天。在索引骨折时未接受骨质疏松症治疗的患者中,60.2%(n=339/563)在骨折后仍未接受治疗,62.2%(n=23/37)在随后骨折后仍未接受治疗。在索引骨折后,83.2%(n=647/778)的患者未进行骨折风险评估(FRAX 或 CAROC),59.9%(n=466/778)的患者未进行骨密度测试。在索引日期前未记录骨质疏松症诊断的患者中,61.3%(n=300/489)在索引骨折后仍未被诊断为骨质疏松症。11.5%(n=86/778)的患者至少发生了一次后续骨折。
在初级保健环境中,脆性骨折很少导致骨质疏松症治疗或骨折风险评估,即使发生多次脆性骨折也是如此。这些结果表明,脆性骨折并未被视为随后骨折的主要危险因素,其发生并未促使初级保健医生进行干预。这些数据促使我们采取措施,识别和克服初级保健医生在脆性骨折后有效管理患者的障碍。