Barutcu Sezgin, Yildirim Abdullah Emre, Sahin Ahmet, Gulsen Murat Taner
Division of Gastroenterology, Gaziantep University Faculty of Medicine, Gaziantep, Turkey.
Department of Infectious Disease and Clinical Microbiology, University of Health Sciences Turkey, Mehmet Akif Inan Research and Training Hospital, Şanlıurfa, Turkey.
Sisli Etfal Hastan Tip Bul. 2022 Mar 28;56(1):77-83. doi: 10.14744/SEMB.2021.58219. eCollection 2022.
The aim of this study was to evaluate the most ideal inflammatory markers for treatment response and to determine a cutoff value that could predict response to treatment for culture negative neutrocytic ascite (CNNA) patients.
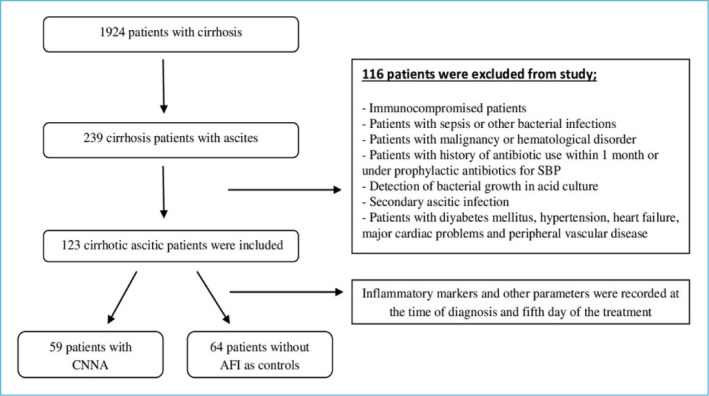
This is a retrospective cross-sectional case-controlled study. Patients with CNNA were evaluated by taking ascites fluid sampling at the beginning and on the 5 day of treatment. Neutrophil-to-lymphocyte ratio (NLR), lymphocyte-to-monocyte ratio (LMR), and neutrophil-to-monocyte ratio were calculated.
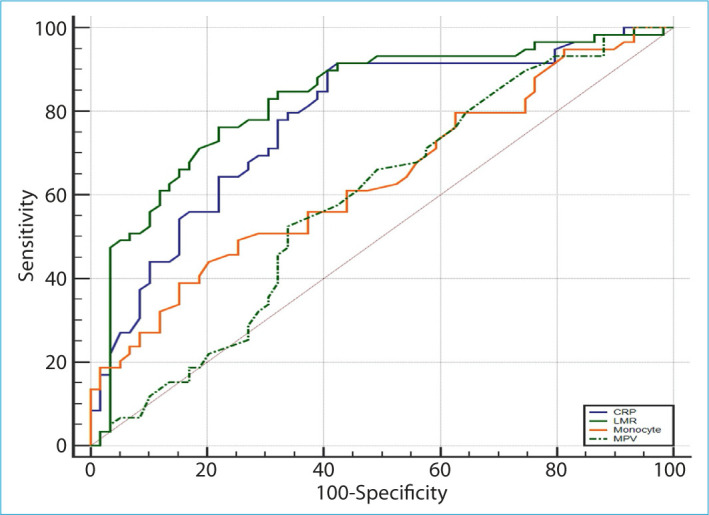
Of the 123 cases with cirrhotic ascites disease, 59 were CCNA and 64 were the control group without ascite-fluid infection. There were statistically significant differences for blood monocyte count, NLR (p<0.01), LMR, and C-reactive protein (CRP) (p<0.001) between two groups. Patients in the CNNA group were compared before and after treatment among themselves for the treatment response. There was statistically significant difference in mean platelet volume, monocyte, LMR, and CRP (p<0.05) between two groups. After receiver operator characteristics curve analysis, the best cutoff value for monocyte was <0.64 × 10/μL (sensitivity 49.2%, specificity 74.6%, positive predictive value [PPV] 65.9%, and negative predictive value [NPV] 59.5%) (p<0.01), for LMR was ≥1.7 (sensitivity 76.3%, specificity 78%, PPV 77.6%, and NPV 76.7%), and for CRP was ≤18 mg/L (sensitivity 91.5% specificity 57.6%, PPV 68.4%, and NPV 87.2%) (p<0.001). When LMR and CRP were used together, sensitivity (86.5%), specificity (83.1%), PPV (83.6%), and NPV (86%) were found to be statistically significantly higher (p<0.001).
Our results showed that in cirrhotic patients with CNNA, combined LMR + CRP can be used as a novel, low cost and non-invasive test to predict treatment response.
本研究旨在评估用于治疗反应的最理想炎症标志物,并确定一个能够预测培养阴性中性粒细胞性腹水(CNNA)患者治疗反应的临界值。
这是一项回顾性横断面病例对照研究。对CNNA患者在治疗开始时和治疗第5天采集腹水样本进行评估。计算中性粒细胞与淋巴细胞比值(NLR)、淋巴细胞与单核细胞比值(LMR)以及中性粒细胞与单核细胞比值。
在123例肝硬化腹水患者中,59例为CNNA患者,64例为无腹水感染的对照组。两组之间血液单核细胞计数、NLR(p<0.01)、LMR和C反应蛋白(CRP)(p<0.001)存在统计学显著差异。对CNNA组患者治疗前后的治疗反应进行自身比较。两组之间平均血小板体积、单核细胞、LMR和CRP存在统计学显著差异(p<0.05)。经过受试者工作特征曲线分析,单核细胞的最佳临界值为<0.64×10/μL(敏感性49.2%,特异性74.6%,阳性预测值[PPV]65.9%,阴性预测值[NPV]59.5%)(p<0.01),LMR的最佳临界值为≥1.7(敏感性76.3%,特异性78%,PPV 77.6%,NPV 76.7%),CRP的最佳临界值为≤18 mg/L(敏感性91.5%,特异性57.6%,PPV 68.4%,NPV 87.2%)(p<0.001)。当联合使用LMR和CRP时,敏感性(86.5%)、特异性(83.1%)、PPV(83.6%)和NPV(86%)在统计学上显著更高(p<0.001)。
我们的结果表明,在患有CNNA的肝硬化患者中,联合LMR + CRP可作为一种新型、低成本且无创的检测方法来预测治疗反应。