Deep Medicine, Nuffield Department of Women's and Reproductive Health, University of Oxford, Hayes House 1F, 75 George St, Oxford, OX1 2BQ, UK.
National Institutes of Health Research Oxford Biomedical Research Centre, Oxford University Hospitals NHS Foundation Trust, Oxford, UK.
Curr Cardiol Rep. 2022 Jul;24(7):851-860. doi: 10.1007/s11886-022-01706-4. Epub 2022 May 7.
To review the recent large-scale randomised evidence on pharmacologic reduction in blood pressure for the primary and secondary prevention of cardiovascular disease.
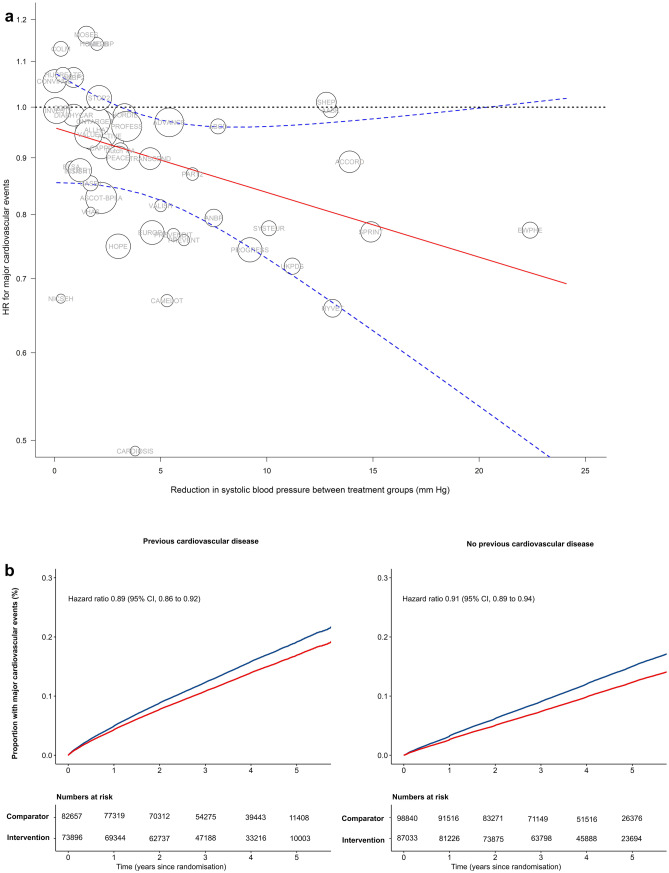
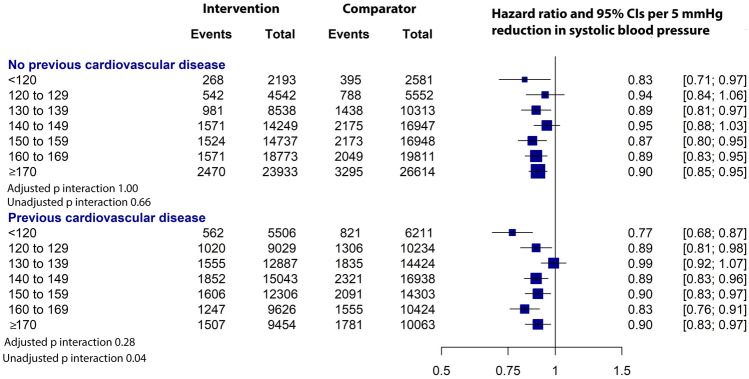
Based on findings of the meta-analysis of individual participant-level data from 48 randomised clinical trials and involving 344,716 participants with mean age of 65 years, the relative reduction in the risk of developing major cardiovascular events was proportional to the magnitude of achieved reduction in blood pressure. For each 5-mmHg reduction in systolic blood pressure, the risk of developing cardiovascular events fell by 10% (hazard ratio [HR] (95% confidence interval [CI], 0.90 [0.88 to 0.92]). When participants were stratified by their history of cardiovascular disease, the HRs (95% CI) in those with and without previous cardiovascular disease were 0.89 (0.86 to 0.92) and 0.91 (0.89 to 0.94), respectively, with no significant heterogeneity in these effects (adjusted P for interaction = 1.0). When these patient groups were further stratified by their baseline systolic blood pressure in increments of 10 mmHg from < 120 to ≥ 170 mmHg, there was no significant heterogeneity in the relative risk reduction across these categories in people with or without previous cardiovascular disease (adjusted P for interaction were 1.00 and 0.28, respectively). Pharmacologic lowering of blood pressure was effective in preventing major cardiovascular disease events both in people with or without previous cardiovascular disease, which was not modified by their baseline blood pressure level. Treatment effects were shown to be proportional to the intensity of blood pressure reduction, but even modest blood pressure reduction, on average, can lead to meaningful gains in the prevention of incident or recurrent cardiovascular disease.
评价降压药物在心血管疾病一级和二级预防中的大型随机对照试验的最新证据。
基于 48 项随机临床试验的个体参与者水平数据的荟萃分析结果,共涉及 344716 名平均年龄为 65 岁的参与者,主要心血管事件风险的降低与血压降低的幅度成正比。收缩压每降低 5mmHg,心血管事件的风险降低 10%(风险比 [HR](95%置信区间 [CI],0.90 [0.88 至 0.92])。按心血管疾病史对参与者分层后,有和无既往心血管疾病者的 HR(95%CI)分别为 0.89(0.86 至 0.92)和 0.91(0.89 至 0.94),这些影响无显著异质性(调整后的交互 P 值=1.0)。当按基线收缩压 10mmHg 递增(<120mmHg 至 ≥170mmHg)进一步分层时,无论基线收缩压水平如何,有或无既往心血管疾病者的相对风险降低幅度均无显著异质性(调整后的交互 P 值分别为 1.00 和 0.28)。降压药物治疗在预防有或无既往心血管疾病者的主要心血管疾病事件中均有效,且不受基线血压水平的影响。降压效果与降压幅度成正比,但即使是平均适度的血压降低,也能在预防新发或复发性心血管疾病方面带来有意义的获益。