Partners In Health, Kigali, Rwanda.
University of Global Health Equity, Butaro, Rwanda.
Int J Equity Health. 2022 May 8;21(1):62. doi: 10.1186/s12939-022-01664-x.
While it is recognized that there are costs associated with postoperative patient follow-up, risk assessments of catastrophic health expenditures (CHEs) due to surgery in sub-Saharan Africa rarely include expenses after discharge. We describe patient-level costs for cesarean section (c-section) and follow-up care up to postoperative day (POD) 30 and evaluate the contribution of follow-up to CHEs in rural Rwanda.
We interviewed women who delivered via c-section at Kirehe District Hospital between September 2019 and February 2020. Expenditure details were captured on an adapted surgical indicator financial survey tool and extracted from the hospital billing system. CHE was defined as health expenditure of ≥ 10% of annual household expenditure. We report the cost of c-section up to 30 days after discharge, the rate of CHE among c-section patients stratified by in-hospital costs and post-discharge follow-up costs, and the main contributors to c-section follow-up costs. We performed a multivariate logistic regression using a backward stepwise process to determine independent predictors of CHE at POD30 at α ≤ 0.05.
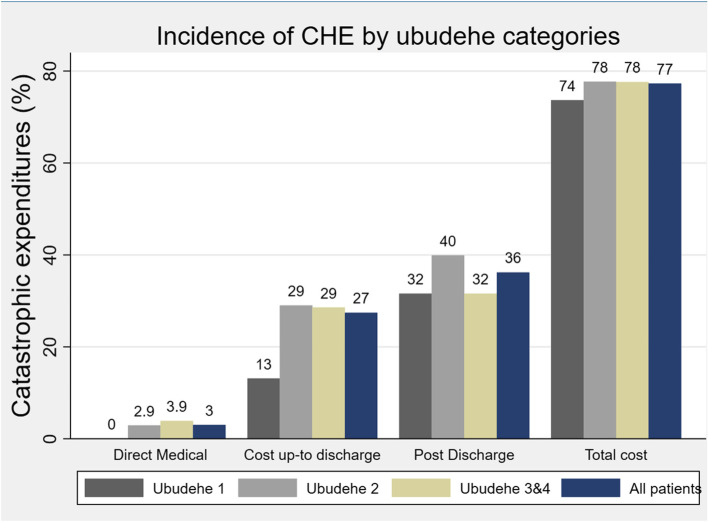
Of the 479 participants in this study, 90% were classified as impoverished before surgery and an additional 6.4% were impoverished by the c-section. The median out-of-pocket costs up to POD30 was US$122.16 (IQR: $102.94, $148.11); 63% of these expenditures were attributed to post-discharge expenses or lost opportunity costs (US$77.50; IQR: $67.70, $95.60). To afford c-section care, 64.4% borrowed money and 18.4% sold possessions. The CHE rate was 27% when only considering direct and indirect costs up to the time of discharge and 77% when including the reported expenses up to POD30. Transportation and lost household wages were the largest contributors to post-discharge costs. Further, CHE at POD30 was independently predicted by membership in community-based health insurance (aOR = 3.40, 95% CI: 1.21,9.60), being a farmer (aOR = 2.25, 95% CI:1.00,3.03), primary school education (aOR = 2.35, 95% CI:1.91,4.66), and small household sizes had 0.22 lower odds of experiencing CHE compared to large households (aOR = 0.78, 95% CI:0.66,0.91).
Costs associated with surgical follow-up are often neglected in financial risk calculations but contribute significantly to the risk of CHE in rural Rwanda. Insurance coverage for direct medical costs is insufficient to protect against CHE. Innovative follow-up solutions to reduce costs of patient transport and compensate for household lost wages need to be considered.
尽管人们认识到术后患者随访会产生成本,但在撒哈拉以南非洲地区,对因手术而导致灾难性医疗支出(CHE)的风险评估很少包括出院后的费用。我们描述了剖宫产(c-section)和术后第 30 天(POD)之前的随访护理的患者层面费用,并评估了随访对卢旺达农村 CHE 的影响。
我们在 2019 年 9 月至 2020 年 2 月期间在基里雷区医院接受剖宫产的女性进行了访谈。支出详情记录在经过修改的手术指标财务调查工具中,并从医院计费系统中提取。 CHE 被定义为医疗支出占家庭年收入的 10%以上。我们报告了出院后 30 天内的剖宫产费用、按住院费用和出院后随访费用分层的剖宫产患者中 CHE 的发生率,以及剖宫产随访费用的主要贡献者。我们使用向后逐步法进行多变量逻辑回归,以确定 POD30 时 CHE 的独立预测因子(α≤0.05)。
在这项研究的 479 名参与者中,90%在手术前被归类为贫困,另有 6.4%因剖宫产而变得贫困。截止到 POD30 的自付费用中位数为 122.16 美元(IQR:102.94 美元,148.11 美元);这些支出中有 63%归因于出院后的费用或机会成本损失(77.50 美元;IQR:67.70 美元,95.60 美元)。为了负担剖宫产护理的费用,64.4%的人借钱,18.4%的人出售财产。仅考虑到出院时的直接和间接费用, CHE 的发生率为 27%,而包括报告的费用至 POD30 时, CHE 的发生率为 77%。交通和家庭工资损失是出院后费用的最大贡献者。此外,社区医疗保险的成员身份(aOR=3.40,95%CI:1.21,9.60)、农民身份(aOR=2.25,95%CI:1.00,3.03)、小学教育(aOR=2.35,95%CI:1.91,4.66)和较小的家庭规模与 CHE 的发生几率较低(aOR=0.78,95%CI:0.66,0.91)。
手术随访相关成本在财务风险计算中经常被忽视,但对卢旺达农村 CHE 的风险有重要影响。直接医疗费用的保险覆盖不足以防止 CHE。需要考虑减少患者交通成本和补偿家庭工资损失的创新随访解决方案。