Liu Zhi-Peng, Chen Wei-Yue, Wang Zi-Ran, Liu Xing-Chao, Fan Hai-Ning, Xu Lei, Pan Yu, Zhong Shi-Yun, Xie Dan, Bai Jie, Jiang Yan, Zhang Yan-Qi, Dai Hai-Su, Chen Zhi-Yu
Department of Hepatobiliary Surgery, Southwest Hospital, Third Military Medical University (Army Medical University), Chongqing, China.
Department of Clinical Research Institute, Lishui Hospital of Zhejiang University, Lishui, China.
Front Oncol. 2022 Apr 21;12:849053. doi: 10.3389/fonc.2022.849053. eCollection 2022.
Recurrence is the main cause of death in perihilar cholangiocarcinoma (pCCA) patients after surgery. Identifying patients with a high risk of recurrence is important for decision-making regarding neoadjuvant therapy to improve long-term outcomes.
The objective of this study was to develop and validate a prognostic model to predict recurrence-free survival (RFS) after curative resection of pCCA.
Patients following curative resection for pCCA from January 2008 to January 2016 were identified from a multicenter database. Using random assignment, 70% of patients were assigned to the training cohort, and the remaining 30% were assigned to the validation cohort. Independent predictors of RFS after curative resection for pCCA were identified and used to construct a prognostic model. The predictive performance of the model was assessed using calibration curves and the C-index.
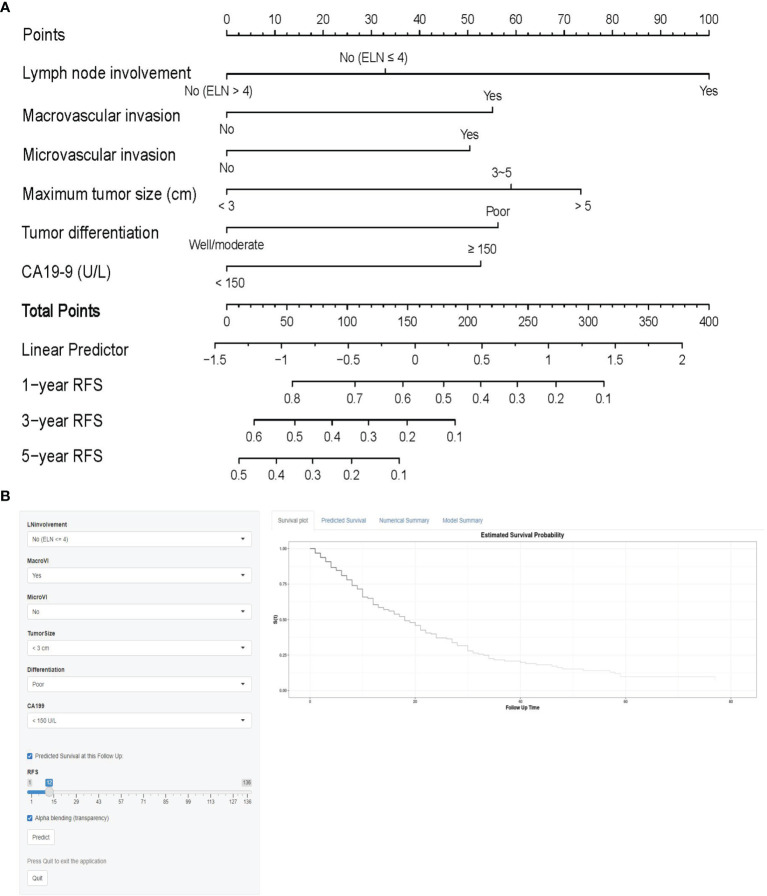
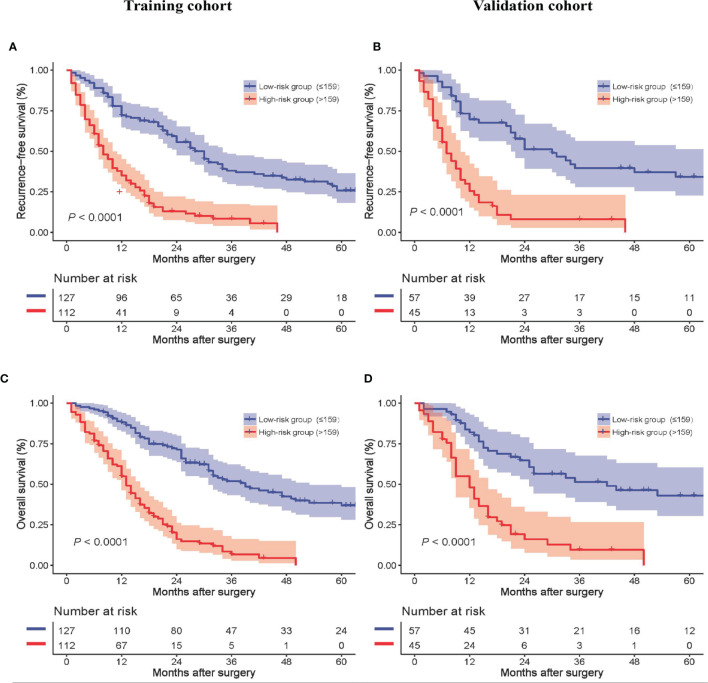
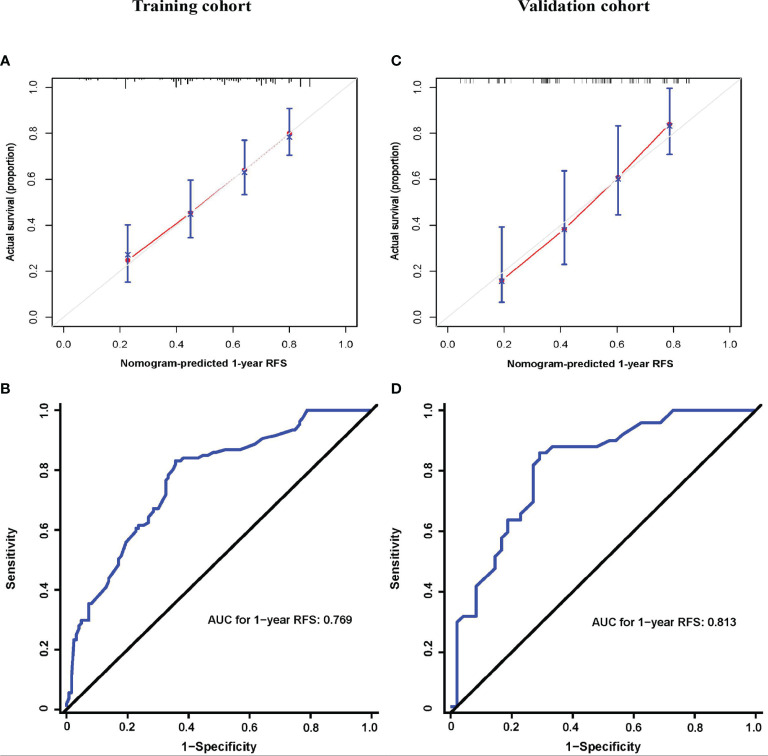
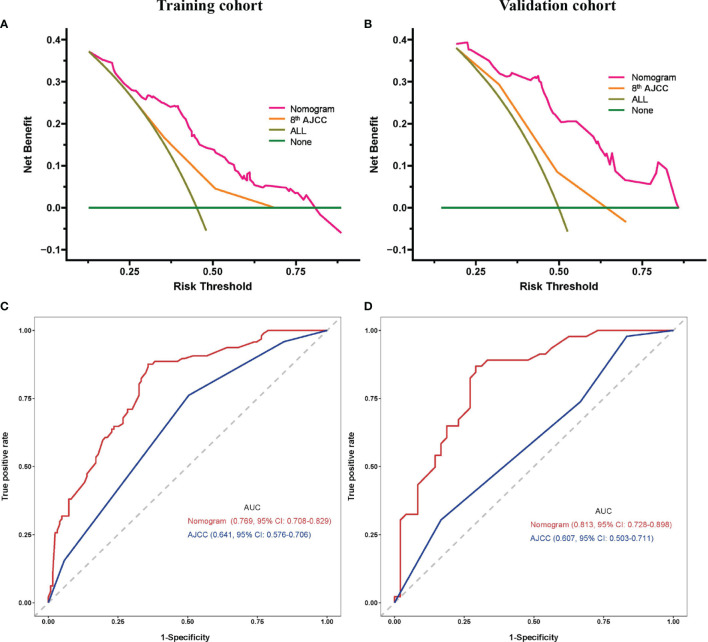
A total of 341 patients were included. The median overall survival (OS) was 22 months, and the median RFS was 14 months. Independent predictors associated with RFS included lymph node involvement, macrovascular invasion, microvascular invasion, maximum tumor size, tumor differentiation, and carbohydrate antigen 19-9. The model incorporating these factors to predict 1-year RFS demonstrated better calibration and better performance than the 8th American Joint Committee on Cancer (AJCC) staging system in both the training and validation cohorts (C-indexes: 0.723 0.641; 0.743 0.607).
The prognostic model could identify patients at high risk of recurrence for pCCA to inform patients and surgeons, help guide decision-making for postoperative adjuvant therapy, and improve survival.
复发是肝门部胆管癌(pCCA)患者术后死亡的主要原因。识别具有高复发风险的患者对于决定新辅助治疗以改善长期预后非常重要。
本研究的目的是开发并验证一种预测模型,以预测pCCA根治性切除术后的无复发生存期(RFS)。
从多中心数据库中确定2008年1月至2016年1月期间接受pCCA根治性切除的患者。通过随机分配,70%的患者被分配到训练队列,其余30%被分配到验证队列。确定pCCA根治性切除术后RFS的独立预测因素,并用于构建预后模型。使用校准曲线和C指数评估该模型的预测性能。
共纳入341例患者。中位总生存期(OS)为22个月,中位RFS为14个月。与RFS相关的独立预测因素包括淋巴结受累、大血管侵犯、微血管侵犯、最大肿瘤大小、肿瘤分化程度和糖类抗原19-9。在训练队列和验证队列中,纳入这些因素预测1年RFS的模型均显示出比美国癌症联合委员会(AJCC)第8版分期系统更好的校准和性能(C指数:训练队列0.723对0.641;验证队列0.743对0.607)。
该预后模型可以识别pCCA高复发风险患者,为患者和外科医生提供信息,帮助指导术后辅助治疗决策,并提高生存率。