Wang Jianping, Huang Manling, Shen Jingxian, Li Bin, Wu Yanqing, Xie Wenxuan, Xiao Han, Tan Li
Department of Gastroenterology and Hepatology, The First Affiliated Hospital, Sun Yat-Sen University, Guangzhou, China.
Department of Oncology, Cancer Center, The First Affiliated Hospital, Sun Yat-Sen University, Guangzhou, China.
Front Surg. 2023 Mar 8;10:1102871. doi: 10.3389/fsurg.2023.1102871. eCollection 2023.
Early-stage intrahepatic cholangiocarcinoma (ESICC) with curative resection and lymph node-negative still has the risk of poor prognosis, and there lacks prognosis-assessing tools for these patients. The objective of this study was to develop a prognosis model to predict outcomes and identify risk stratification for ESICC after resection.
Totally 263 patients with ESICC after hepatectomy from January 2012 to January 2022 were analyzed. Clinicopathological factors were selected using multivariable Cox regression analysis and a prognosis model was developed. The performance of the model was evaluated by concordance index (C-index), calibration plots, decision curves analysis (DCA), and net reclassification index (NRI). Kaplan-Meier curves were analyzed for risk stratification of overall survival (OS) and recurrence-free survival (RFS) based on the prognosis model.
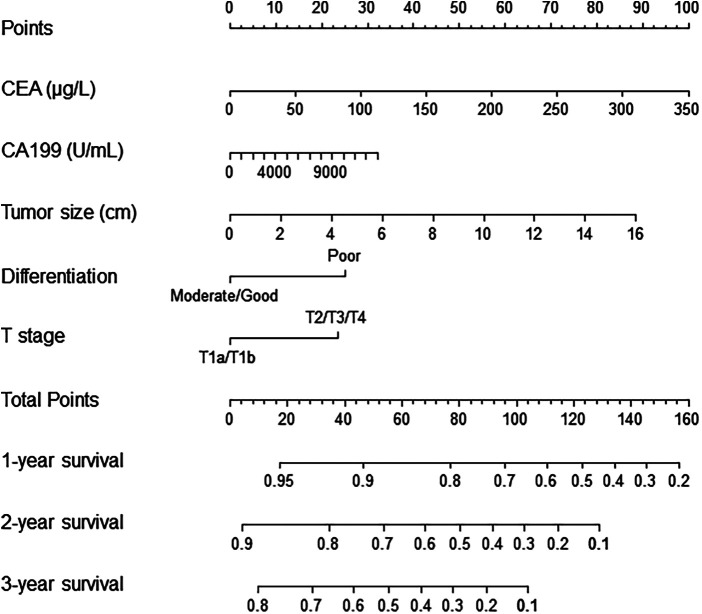
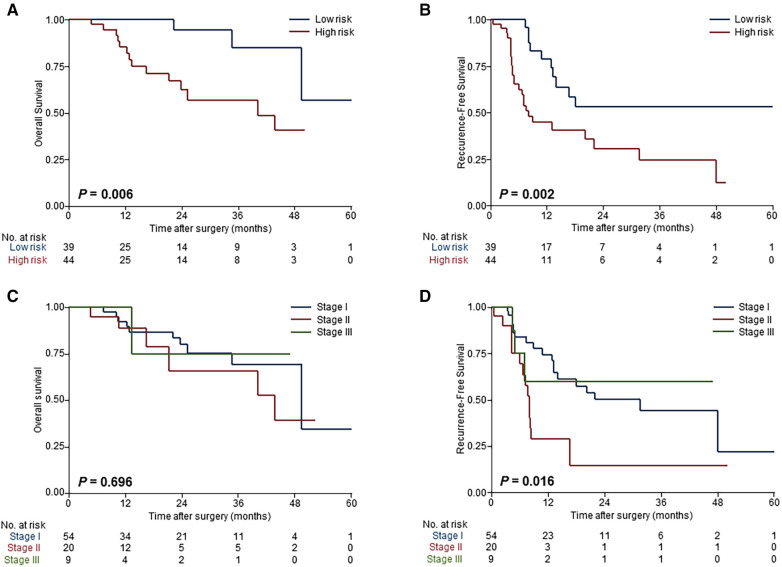
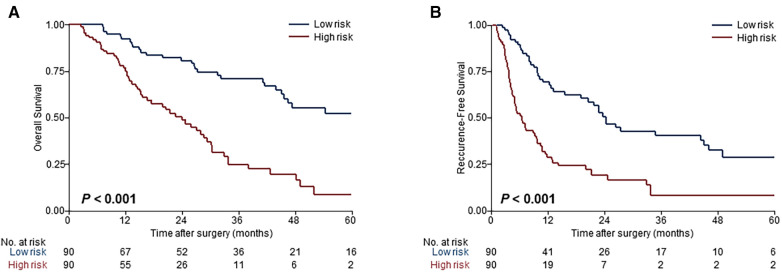
The clinicopathological features that were independently associated with OS of ESICC included carbohydrate antigen19-9, carcinoembryonic antigen, tumor size, tumor differentiation, and T stage. The prognosis model based on these prognostic factors demonstrated excellent discriminatory performance in both derivation cohort (C-index, 0.71) and external validation cohort (C-index, 0.78), which outperformed the TNM staging system (C-index, 0.59) and individual prognostic factors (all C-index < 0.7). Calibration plots, DCA and NRI also showed superior predictive performance. According to the risk for survival, the model stratified patients into low risk (median OS, 66.6 months; median RFS, 24.3 months) and high risk (median OS, 24.0 months; median RFS, 6.4 months) ( 0.001).
Our prognosis model can robustly predict the outcomes of ESICC after curative resection and provide precise evaluation on prognosis risk, facilitating clinicians to develop individualized postoperative treatment options.
接受根治性切除且淋巴结阴性的早期肝内胆管癌(ESICC)仍有预后不良的风险,且缺乏针对这些患者的预后评估工具。本研究的目的是建立一个预后模型,以预测ESICC切除术后的结局并确定风险分层。
分析了2012年1月至2022年1月期间263例肝切除术后的ESICC患者。采用多变量Cox回归分析选择临床病理因素,并建立预后模型。通过一致性指数(C指数)、校准曲线、决策曲线分析(DCA)和净重新分类指数(NRI)评估模型的性能。基于预后模型分析Kaplan-Meier曲线,对总生存期(OS)和无复发生存期(RFS)进行风险分层。
与ESICC的OS独立相关的临床病理特征包括糖类抗原19-9、癌胚抗原、肿瘤大小、肿瘤分化和T分期。基于这些预后因素的预后模型在推导队列(C指数,0.71)和外部验证队列(C指数,0.78)中均表现出优异的鉴别性能,优于TNM分期系统(C指数,0.59)和个体预后因素(所有C指数<0.7)。校准曲线、DCA和NRI也显示出优越的预测性能。根据生存风险,该模型将患者分为低风险(中位OS,66.6个月;中位RFS,24.3个月)和高风险(中位OS,24.0个月;中位RFS,6.4个月)(P<0.001)。
我们的预后模型能够可靠地预测ESICC根治性切除术后的结局,并对预后风险进行精确评估,有助于临床医生制定个体化的术后治疗方案。