Pharmacy Department, Austin Health, Victoria, Australia.
Centre for Medicine Use and Safety, Faculty of Pharmacy and Pharmaceutical Sciences, Monash University, Victoria, Australia.
Br J Clin Pharmacol. 2022 Oct;88(10):4565-4572. doi: 10.1111/bcp.15394. Epub 2022 May 23.
To describe paracetamol dosing and liver function test (LFT) monitoring in older hospital inpatients who are frail or have low body weight.
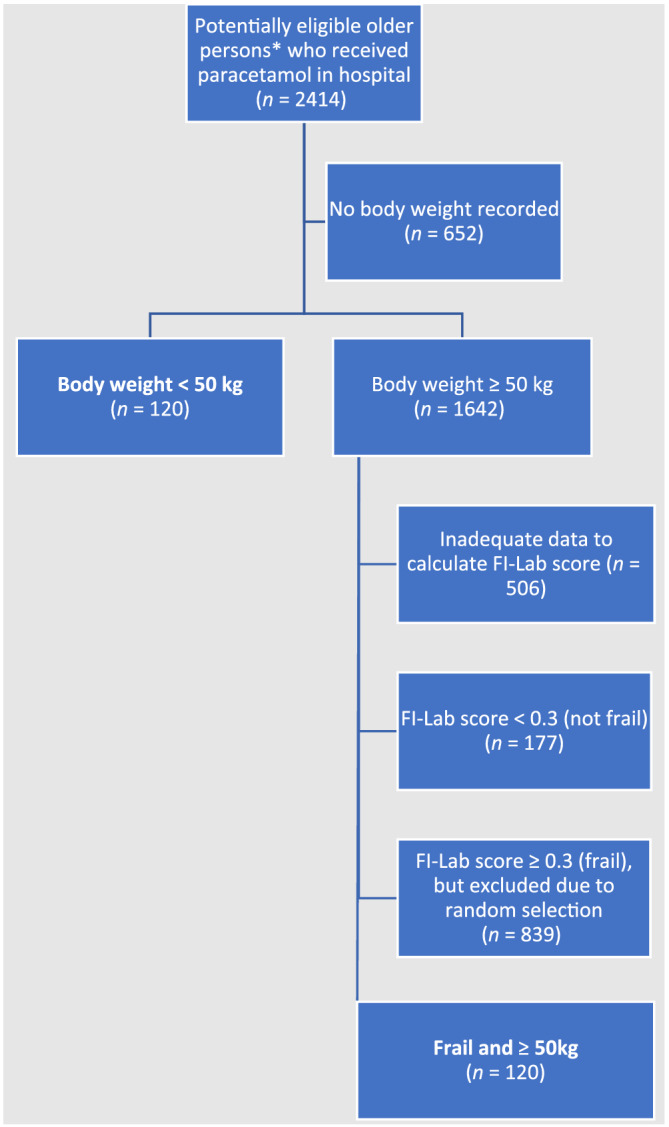
Retrospective observational study, at a 790-bed metropolitan public health service in Australia. Patients aged ≥70 years, with body weight <50 kg or frailty index based on laboratory data (FI-Lab) score ≥0.3, who were administered paracetamol during an admission with length-of-stay >72 hours, were included. Data were extracted from electronic medical records. Paracetamol doses administered in hospital, and doses prescribed on discharge, were compared against consensus guidelines that recommended ≤60 mg/kg/d for older people weighing <50 kg, and ≤3000 mg/d for frail older people.
In total, 240 admissions (n = 229 patients, mean age 84.7 years) were analysed. During 150 (62.5%) admissions, higher than recommended paracetamol doses were prescribed. On 138 (57.5%) occasions, patients were prescribed paracetamol on discharge, and 112/138 (81.2%) doses were higher than recommended. Most discharge prescriptions (97/138, 70.3%) were for regular administration. The median daily dose on discharge for patients <50 kg was 83.7 mg/kg (interquartile range 73.6-90.9 mg/kg). For frail patients ≥50 kg, the median daily discharge dose was 3990 mg (interquartile range 3000-4000 mg). LFTs were measured in hospital for 151/200 (75.5%) and 93/166 (56.0%) patients who received paracetamol for >48 hours and >5 days, respectively.
Majority of paracetamol doses prescribed for frail or low-weight older patients in hospital and on discharge were higher than recommended in consensus guidelines. LFTs were not measured for 44% patients who received paracetamol regularly for >5 days. Further studies are needed to explore long-term outcomes of this practice.
描述在体弱或体重较低的老年住院患者中,扑热息痛的剂量和肝功能检查(LFT)监测情况。
这是一项在澳大利亚一家拥有 790 张床位的大都市公立卫生服务机构开展的回顾性观察性研究。纳入年龄≥70 岁、体重<50kg 或基于实验室数据(FI-Lab)评分≥0.3 的虚弱指数的患者,这些患者在住院时间>72 小时的入院期间接受了扑热息痛治疗。数据从电子病历中提取。比较了在医院给予的扑热息痛剂量和出院时开具的剂量与建议的共识指南,建议体重<50kg 的老年人≤60mg/kg/d,体弱老年人≤3000mg/d。
共分析了 240 例入院(n=229 例患者,平均年龄 84.7 岁)。在 150 例(62.5%)入院中,开具了高于建议的扑热息痛剂量。在 138 例(57.5%)情况下,患者出院时开具了扑热息痛处方,其中 112/138(81.2%)剂量高于建议。大多数出院处方(97/138,70.3%)为常规给药。体重<50kg 的患者出院时的平均每日剂量为 83.7mg/kg(中位数范围为 73.6-90.9mg/kg)。对于≥50kg 的虚弱患者,出院时的中位每日剂量为 3990mg(中位数范围为 3000-4000mg)。在接受扑热息痛治疗>48 小时和>5 天的 151/200(75.5%)和 93/166(56.0%)患者中,分别有 151/200(75.5%)和 93/166(56.0%)在医院和出院时测量了肝功能检查。
在体弱或体重较低的老年住院患者中,医院和出院时开具的扑热息痛剂量有很大一部分高于共识指南建议。对于>5 天常规接受扑热息痛治疗的 44%患者,未测量肝功能检查。需要进一步研究以探讨这种做法的长期结果。