Muhammad Milan, Ayton Sarah, Hejmadi Shruthi, Minhas Jatinder S, Morgan Nicolette, Peek Anna C
Department of Trauma and Orthopaedics, University Hospitals of Leicester, Infirmary Square, Leicester, LE1 5WW, UK.
Department of Elderly Medicine, University Hospitals of Leicester, Leicester, UK.
J Clin Orthop Trauma. 2022 Jun;29:101890. doi: 10.1016/j.jcot.2022.101890. Epub 2022 May 6.
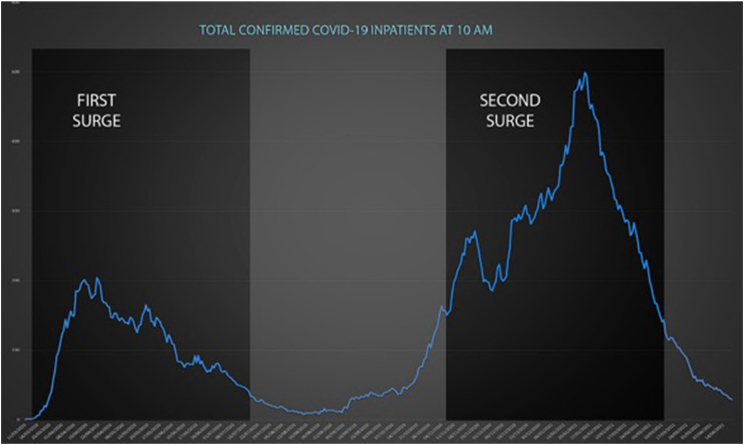
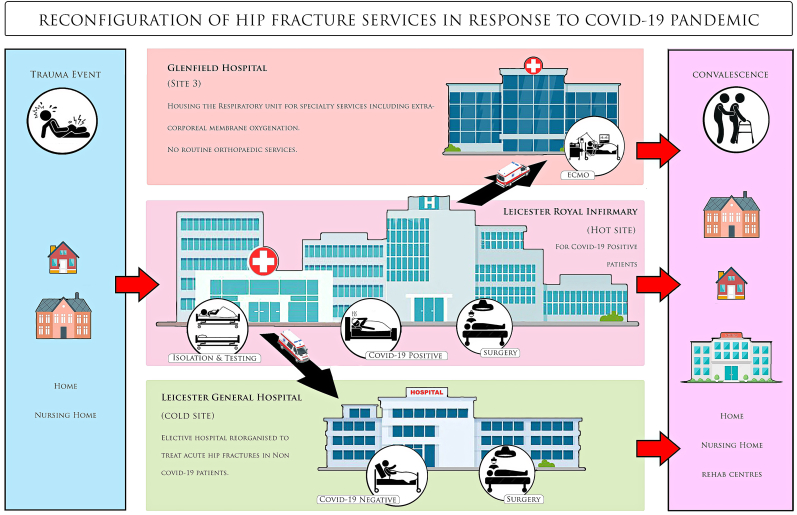
The Covid-19 pandemic has had an unprecedented effect on surgical practice and healthcare delivery globally. We compared the impact of the care pathways which segregate Covid-19 Positive and Negative patients into two geographically separate sites, on hip fracture patients in our high-volume trauma center in 3 distinct eras - the pre-pandemic period, against the first Covid-19 wave with dual-site service design, as well as the subsequent surge with single-site service delivery. In addition, we sought to invoke similar experiences of centres worldwide through a scoping literature review on the current evidence on "Dual site" reconfigurations in response to Covid-19 pandemic.
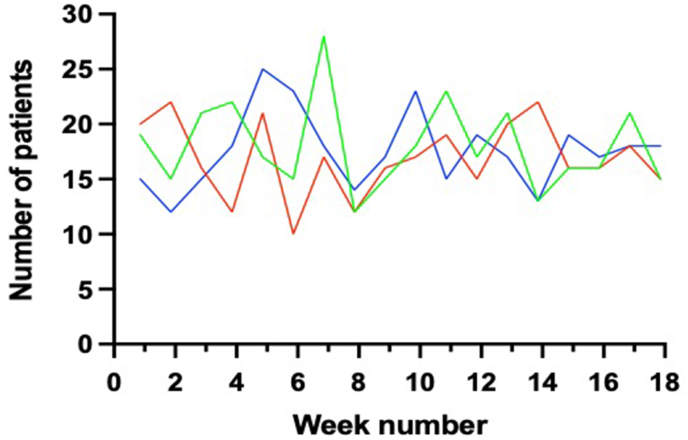
We prospectively reviewed our hip fracture patients throughout the two peaks of the pandemic, with different service designs for each, and compared the outcomes with a historic service provision. Further, a comprehensive literature search was conducted using several databases for articles discussing Dual-site service redesign.
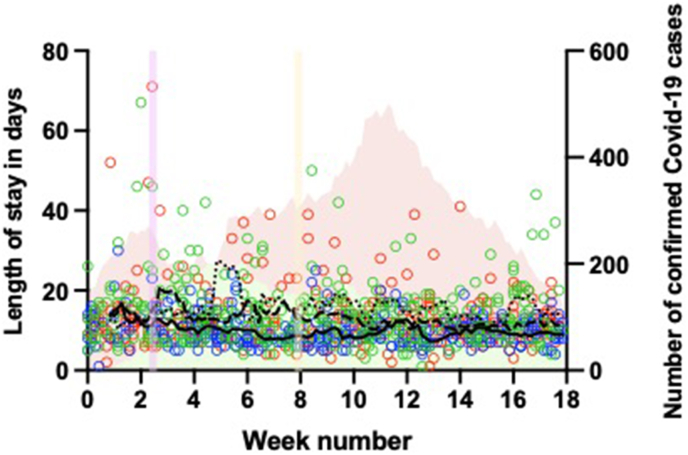
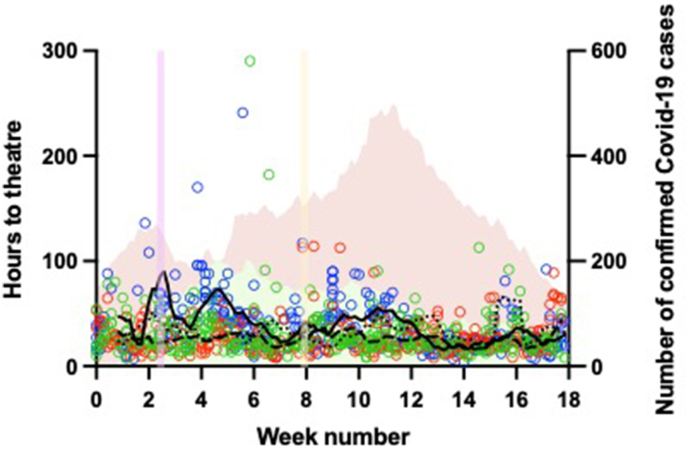
In our in-house study, there was no statistically significant difference in mortality of hip fracture patients between the 3 periods, as well as their discharge destinations. With dual-site reconfiguration, patients took longer to reach theatre. However, there was much more nosocomial transmission with single-site service, and patients stayed in the hospital longer. 24 articles pertaining to the topic were selected for the scoping review. Most studies favour dual-site service reorganization, and reported beneficial outcomes from the detached care pathways.
It is safe to continue urgent as well as non-emergency surgery during the Covid-19 pandemic in a separate, geographically isolated site.
新冠疫情对全球外科手术实践和医疗服务产生了前所未有的影响。我们比较了在三个不同时期,即疫情前时期、新冠疫情第一波期间采用双院区服务设计以及随后单院区服务提供期间,将新冠阳性和阴性患者分置于两个地理位置不同的院区的护理路径,对我们高流量创伤中心髋部骨折患者的影响。此外,我们通过对当前关于应对新冠疫情的“双院区”重新配置的证据进行范围界定文献综述,试图援引全球各中心的类似经验。
我们前瞻性地回顾了疫情两个高峰期的髋部骨折患者,每个时期采用不同的服务设计,并将结果与历史服务提供情况进行比较。此外,使用多个数据库进行了全面的文献检索,以查找讨论双院区服务重新设计的文章。
在我们的内部研究中,三个时期髋部骨折患者的死亡率及其出院去向没有统计学上的显著差异。采用双院区重新配置时,患者到达手术室的时间更长。然而,单院区服务的医院内传播更多,患者住院时间更长。我们选择了24篇与该主题相关的文章进行范围界定综述。大多数研究倾向于双院区服务重组,并报告了分离护理路径带来的有益结果。
在新冠疫情期间,在一个单独的、地理位置隔离的院区继续进行急诊和非急诊手术是安全的。